
How to select the right speech language pathologist for your adopted child?
You have decided to consult a private speech language pathologist because of concerns over your adopted child’s developing speech and language. But how do you choose the right one? There are many speech therapists out there and not all of them are alike in experience and skills. On top of it all, you are also looking for a bilingual therapist, one who is not only proficient in your child’s native language but is also knowledgeable regarding the speech and language issues of international adoptees. That is not an easy decision to make, especially for many parents who until now have not had any direct contact with a speech language pathologist.
Not to worry, below is a list of simple guidelines designed to assist you in the right therapist selection.
Let’s begin with something basic: educational and professional credentials. A speech language pathologist must possess a Master’s Degree (or its equivalent) from a reputable academic institution of higher learning. They must also have a Certificate of Clinical Competence from the American Speech Language Hearing Association as well as an appropriate licensure from the state in which they maintain their practice. Additionally, it is highly recommended that they have Bilingual Certification as it indicates that they have completed the necessary academic coursework and are proficient in the issues surrounding normal and disordered speech-language acquisition of bilingual children in dual languages.
Now we are ready to proceed to experience. Here its gets a little tricky. The traditional approach: “I want the therapist with a gazillion years of experience” is just not going to be all that useful. It can’t be just any experience; it has to be the right experience! After all do you really want a therapist with 30 years of experience in exclusively treating articulation deficits when your child needs help with feeding and swallowing or with developing augmentative/alternative communication?
It is important to choose a therapist who has a rich and varied experience from multiple settings, total years of experience may not be as important as the qualitative value of that experience. A good therapist has probably spent a considerable portion of his/her time in a variety of settings from schools and early intervention agencies to hospitals and rehabilitation clinics. As the result of working in these diverse environments that therapist is much more likely to come up with innovative ideas and solutions to your child’s problems as opposed to just using the same old remediation strategies that they have learned way back then. It is also a good idea to inquire regarding the areas of specialization of the therapist in order to find out whether he/she has successfully treated children with similar problems to your child’s.
Typically, private speech language pathologists who maintain some type of pediatric hospital affiliation (e.g. per diem or part-time employees) are up to date regarding the current methodologies, which they apply to practice on daily basis. The reasons for that are twofold:
Speech departments in hospitals deal with diverse caseloads, with patients ranging in ages, diagnoses (some of which can be quite unusual), and levels of severity. In an average inpatient department staff SLP’s are expected to carry caseloads of 12-16 patients per day.
In order to keep up with the caseload diversity and with the latest treatment trends, hospitals require these SLP’s to actively take professional development courses in order to provide their patients with the best quality of care.
This brings us to another important consideration: professional development. To maintain their state licensure and national certification all therapists are required to take professional education courses in order to stay up to date with all the relevant research and new treatments developed in our field. The minimum requirement is to accumulate 30 professional education hours every 3 years whether by attending courses in person, taking them online through qualified providers, or by conducting workshops and presenting at conferences. Professional development provides the speech therapists with an opportunity to use evidence based techniques supported and tested by research to treat a variety of communication disorders. Consequently, when selecting your therapist it is important to find out just how up to date are they on the current treatment methods and methodologies pertaining to your child speech and language deficits. You can always find out this information by politely questioning the therapist regarding their background and “resume highlights.”
It is also important to find out whether you understand and agree with the therapist’s methods and approaches. For example, if your child is a toddler, it probably does not make sense for him/her to spend most sessions doing worksheets and drills when he/she needs to be engaged in play based, child centered therapy. Don’t be intimidated by the therapist’s credentials and your lack of knowledge, if something they said doesn’t make sense, ask follow up questions and/or look up pertinent information online. While you should not use the internet to diagnose your child’s problems, it can be used as a valuable learning tool to look up information and to share ideas with other parents who experience similar difficulties.
Now that we have specified general selection criteria, let’s talk about how to initiate your search for the right SLP. The best way is again to go online. Start your search by going to the ASHA website and clicking on the ‘Find Professional Button’ located in the top of the page and then follow the instructions on the screen. Fill out your search criteria carefully but don’t be too specific. For example, don’t look for a Russian speaking SLP in Blue Creek, California as you will probably not find one. Instead try typing in the first 3 digits of your zipcode or your state of residence (if it’s small enough) and don’t forget to specify the language of the practitioner. That will get you the optimum results.
Once you have located several candidates, you can narrow down the search by trying to learn something about them online. Google the clinician’s name (or the name of their practice) to see whether they have their own website, have written any articles or have been profiled by any organizations. To make sure that your practitioner’s licensure is up to date, visit your state’s speech language accreditation website and type in the last name of the professional. Typically, a window will pop up listing the therapists’ names alphabetically, find the one you are looking for and check if their license is active. Finally, armed with your research, create a list of questions that you might have for the practitioners and start making phone calls. Find out all the pertinent information and don’t forget to ask about rates which may differ depending on what services the practitioner is providing.
Please note that many private practitioners refuse to deal with insurance companies directly due to the hassle of multiclient billing as well as extended wait for reimbursement. They will instead provide you with a letter for your insurance company, containing the necessary diagnosis and treatment codes, incurred fees as well as a brief description of services provided, and will expect you to apply for reimbursement on your own.
Now that we have gone over the selection process in some detail, please keep in mind that you can always learn more information on this and any other speech pathology related topic by visiting the ASHA website and clicking on the ‘Public’ tab located at the top of the screen.
Best of luck in your search and happy hunting!
Useful websites:
Find a Professional SLP on the ASHA website: http://www.asha.org/proserv/
State Contacts & Licensure Requirements: http://www.asha.org/about/legislation-advocacy/state/
 In the past several years, due to an influx of adolescent students with language and learning difficulties on my caseload, I have begun to research in depth aspects of adolescent
In the past several years, due to an influx of adolescent students with language and learning difficulties on my caseload, I have begun to research in depth aspects of adolescent  For this purpose, I often use the books from the Continental Press series entitled:
For this purpose, I often use the books from the Continental Press series entitled: 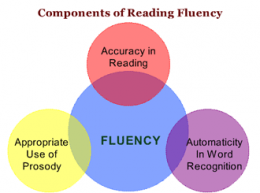 Reading Fluency: TS’s reading fluency (automaticity, prosody, accuracy and speed, expression, intonation, and phrasing) during the reading task was marked by monotone vocal quality, awkward word stress, imprecise articulatory contacts, false-starts, self–revisions, awkward mid-sentential pauses, limited pausing for punctuation, as well as misreadings and word substitutions, all of which resulted in an impaired reading prosody.
Reading Fluency: TS’s reading fluency (automaticity, prosody, accuracy and speed, expression, intonation, and phrasing) during the reading task was marked by monotone vocal quality, awkward word stress, imprecise articulatory contacts, false-starts, self–revisions, awkward mid-sentential pauses, limited pausing for punctuation, as well as misreadings and word substitutions, all of which resulted in an impaired reading prosody. Text Vocabulary Comprehension:
Text Vocabulary Comprehension: Impressions: Clinical below grade-level reading comprehension assessment reading revealed that TS presents with a number of reading related difficulties. TS’s reading fluency was marked by monotone vocal quality, awkward word stress, imprecise articulatory contacts, false-starts, self–revisions, awkward mid-sentential pauses, limited pausing for punctuation, as well as misreadings and word substitutions, all of which resulted in an impaired reading prosody. TS’s understanding as well as his verbal summary of the presented text was immature for his age and was characterized by impaired gestalt processing of information resulting in an ineffective and confusing summarization. While TS’s text-based vocabulary knowledge was deemed to be grossly adequate for his age, his reading comprehension abilities were judged to be impaired for his age. Therapeutic intervention is strongly recommended to improve TS’s reading abilities. (See Impressions and Recommendations sections for further details).
Impressions: Clinical below grade-level reading comprehension assessment reading revealed that TS presents with a number of reading related difficulties. TS’s reading fluency was marked by monotone vocal quality, awkward word stress, imprecise articulatory contacts, false-starts, self–revisions, awkward mid-sentential pauses, limited pausing for punctuation, as well as misreadings and word substitutions, all of which resulted in an impaired reading prosody. TS’s understanding as well as his verbal summary of the presented text was immature for his age and was characterized by impaired gestalt processing of information resulting in an ineffective and confusing summarization. While TS’s text-based vocabulary knowledge was deemed to be grossly adequate for his age, his reading comprehension abilities were judged to be impaired for his age. Therapeutic intervention is strongly recommended to improve TS’s reading abilities. (See Impressions and Recommendations sections for further details). Recently I wrote a blog post regarding how SLPs can
Recently I wrote a blog post regarding how SLPs can 
 Now let us select a few writing goals for this student.
Now let us select a few writing goals for this student.


 Lately I’ve had a number of children on my caseload with marked cognitive limitations. While I always attempt to integrate curriculum concepts into their therapy sessions, I also focus extensively on doing functional activities with them. These are tasks that pertain to daily living such as ordering food in a restaurant, shopping in supermarket, performing household activities, or looking up information. This is why I was very happy to come across
Lately I’ve had a number of children on my caseload with marked cognitive limitations. While I always attempt to integrate curriculum concepts into their therapy sessions, I also focus extensively on doing functional activities with them. These are tasks that pertain to daily living such as ordering food in a restaurant, shopping in supermarket, performing household activities, or looking up information. This is why I was very happy to come across  My birthday month has been absolutely fabulous! And its not over yet! So take a look at the Week Four Giveaway Lineup and decide whether you want to enter a few giveaways or all of them, it’s really up to you! Each giveaway will last only one day so you better keep up because if you blink you’ll miss it!
My birthday month has been absolutely fabulous! And its not over yet! So take a look at the Week Four Giveaway Lineup and decide whether you want to enter a few giveaways or all of them, it’s really up to you! Each giveaway will last only one day so you better keep up because if you blink you’ll miss it!
 A few days ago I was asked by my higher-ups for a second opinion on a consult regarding a psychological evaluation on an 11-year-old boy, which was depicting a certain pattern of deficits without a reasonable justification as to why they were occurring. I had a working hypothesis but needed more evidence to turn it into a viable theory. So I set out to collect more evidence by interviewing a few ancillary professionals who were providing therapy services to the student.
A few days ago I was asked by my higher-ups for a second opinion on a consult regarding a psychological evaluation on an 11-year-old boy, which was depicting a certain pattern of deficits without a reasonable justification as to why they were occurring. I had a working hypothesis but needed more evidence to turn it into a viable theory. So I set out to collect more evidence by interviewing a few ancillary professionals who were providing therapy services to the student.


 Today I am a reviewing a new vocabulary app created by the Virtual Speech Center called
Today I am a reviewing a new vocabulary app created by the Virtual Speech Center called 
 Here is the problem though: I only see the above follow-up steps in a small percentage of cases. In the vast majority of cases in which score discrepancies occur, I see the examiners ignoring the weaknesses without follow up. This of course results in the child not qualifying for services.
Here is the problem though: I only see the above follow-up steps in a small percentage of cases. In the vast majority of cases in which score discrepancies occur, I see the examiners ignoring the weaknesses without follow up. This of course results in the child not qualifying for services. So the next time you see a pattern of strengths and weaknesses and testing, even if it amounts to a total average score, I urge you to dig deeper. I urge you to investigate why this pattern is displayed in the first place. The same goes for you – parents! If you are looking at average total scores but seeing unexplained weaknesses in select testing areas, start asking questions! Ask the professional to explain why those deficits are occuring and tell them to dig deeper if you are not satisfied with what you are hearing. All students deserve access to FAPE (Free and Appropriate Public Education). This includes access to appropriate therapies, they may need in order to optimally function in the classroom.
So the next time you see a pattern of strengths and weaknesses and testing, even if it amounts to a total average score, I urge you to dig deeper. I urge you to investigate why this pattern is displayed in the first place. The same goes for you – parents! If you are looking at average total scores but seeing unexplained weaknesses in select testing areas, start asking questions! Ask the professional to explain why those deficits are occuring and tell them to dig deeper if you are not satisfied with what you are hearing. All students deserve access to FAPE (Free and Appropriate Public Education). This includes access to appropriate therapies, they may need in order to optimally function in the classroom.