 As a speech-language pathologist (SLP) working in a psychiatric setting, I routinely address social pragmatic language goals as part of my clinical practice. Finding the right approach to the treatment of social pragmatic language disorders has been challenging to say the least. That is because the efficacy of social communication interventions continues to be quite limited. Studies to date continue to show questionable results and limited carryover, while measurements of improvement are frequently subjective, biased, and subject to a placebo effect, maturation effect, and regression to the mean. However, despite the significant challenges to clinical practice in this area, the usage of videos for treatment purposes shows an emergent promise. Continue reading On the Value of Social Pragmatic Interventions via Video Analysis
As a speech-language pathologist (SLP) working in a psychiatric setting, I routinely address social pragmatic language goals as part of my clinical practice. Finding the right approach to the treatment of social pragmatic language disorders has been challenging to say the least. That is because the efficacy of social communication interventions continues to be quite limited. Studies to date continue to show questionable results and limited carryover, while measurements of improvement are frequently subjective, biased, and subject to a placebo effect, maturation effect, and regression to the mean. However, despite the significant challenges to clinical practice in this area, the usage of videos for treatment purposes shows an emergent promise. Continue reading On the Value of Social Pragmatic Interventions via Video Analysis
Category: emotional and behavioral disturbances
Clinical Fellow (and Setting-Switching SLPs) Survival Guide in the Schools
 It’s early August, and that means that the start of a new school year is just around the corner. It also means that many newly graduated clinical fellows (as well as SLPs switching their settings) will begin their exciting yet slightly terrifying new jobs working for various school systems around the country. Since I was recently interviewing clinical fellows myself in my setting (an outpatient school located in a psychiatric hospital, run by a university), I decided to write this post in order to assist new graduates, and setting-switching professionals by describing what knowledge and skills are desirable to possess when working in the schools. Continue reading Clinical Fellow (and Setting-Switching SLPs) Survival Guide in the Schools
It’s early August, and that means that the start of a new school year is just around the corner. It also means that many newly graduated clinical fellows (as well as SLPs switching their settings) will begin their exciting yet slightly terrifying new jobs working for various school systems around the country. Since I was recently interviewing clinical fellows myself in my setting (an outpatient school located in a psychiatric hospital, run by a university), I decided to write this post in order to assist new graduates, and setting-switching professionals by describing what knowledge and skills are desirable to possess when working in the schools. Continue reading Clinical Fellow (and Setting-Switching SLPs) Survival Guide in the Schools
Test Review: Clinical Assessment of Pragmatics (CAPs)
 Today due to popular demand I am reviewing the Clinical Assessment of Pragmatics (CAPs) for children and young adults ages 7 – 18, developed by the Lavi Institute and sold by WPS Publishing. Readers of this blog are familiar with the fact that I specialize in working with children diagnosed with psychiatric impairments and behavioral and emotional difficulties. They are also aware that I am constantly on the lookout for good quality social communication assessments due to a notorious dearth of good quality instruments in this area of language. Continue reading Test Review: Clinical Assessment of Pragmatics (CAPs)
Today due to popular demand I am reviewing the Clinical Assessment of Pragmatics (CAPs) for children and young adults ages 7 – 18, developed by the Lavi Institute and sold by WPS Publishing. Readers of this blog are familiar with the fact that I specialize in working with children diagnosed with psychiatric impairments and behavioral and emotional difficulties. They are also aware that I am constantly on the lookout for good quality social communication assessments due to a notorious dearth of good quality instruments in this area of language. Continue reading Test Review: Clinical Assessment of Pragmatics (CAPs)
Using Picture Books to Teach Children That It’s OK to Make Mistakes and Take Risks
 Those of you who follow my blog know that in my primary job as an SLP working for a psychiatric hospital, I assess and treat language and literacy impaired students with significant emotional and behavioral disturbances. I often do so via the aid of picture books (click HERE for my previous posts on this topic) dealing with a variety of social communication topics. Continue reading Using Picture Books to Teach Children That It’s OK to Make Mistakes and Take Risks
Those of you who follow my blog know that in my primary job as an SLP working for a psychiatric hospital, I assess and treat language and literacy impaired students with significant emotional and behavioral disturbances. I often do so via the aid of picture books (click HERE for my previous posts on this topic) dealing with a variety of social communication topics. Continue reading Using Picture Books to Teach Children That It’s OK to Make Mistakes and Take Risks
Speech, Language, and Literacy Fun with Helen Lester’s Picture Books
 Picture books are absolutely wonderful for both assessment and treatment purposes! They are terrific as narrative elicitation aids for children of various ages, ranging from pre-K through fourth grade. They are amazing treatment aids for addressing a variety of speech, language, and literacy goals that extend far beyond narrative production. Continue reading Speech, Language, and Literacy Fun with Helen Lester’s Picture Books
Picture books are absolutely wonderful for both assessment and treatment purposes! They are terrific as narrative elicitation aids for children of various ages, ranging from pre-K through fourth grade. They are amazing treatment aids for addressing a variety of speech, language, and literacy goals that extend far beyond narrative production. Continue reading Speech, Language, and Literacy Fun with Helen Lester’s Picture Books
Assessing Social Pragmatic Abilities in Children with Language Difficulties
You’ve received a referral to assess the language abilities of a school aged child with suspected language difficulties. The child has not been assessed before so you know you’ll need a comprehensive language test to look at the child’s ability to recall sentences, follow directions, name words, as well as perform a number of other tasks showcasing the child’s abilities in the areas of content and form (Bloom & Lahey, 1978).
But how about the area of language use? Will you be assessing the child’s pragmatic and social cognitive abilities as well during your language assessment? After all most comprehensive standardized assessments, “typically focus on semantics, syntax, morphology, and phonology, as these are the performance areas in which specific skill development can be most objectively measured” (Hill & Coufal, 2005, p 35). Continue reading Assessing Social Pragmatic Abilities in Children with Language Difficulties
Dear SLPs, Here’s What You Need to Know About Internationally Adopted Children
 In the past several years there has been a sharp decline in international adoptions. Whereas in 2004, Americans adopted a record high of 22,989 children from overseas, in 2015, only 5,647 children (a record low in 30 years) were adopted from abroad by American citizens.
In the past several years there has been a sharp decline in international adoptions. Whereas in 2004, Americans adopted a record high of 22,989 children from overseas, in 2015, only 5,647 children (a record low in 30 years) were adopted from abroad by American citizens.
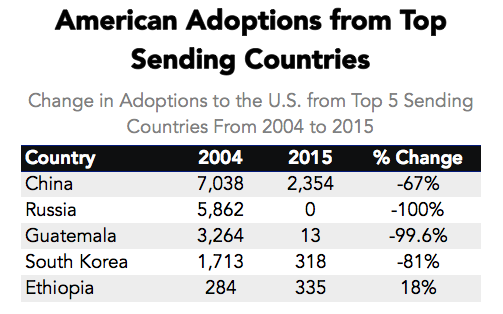
Primary Data Source: Data Source: U.S. State Department Intercountry Adoption Statistics
Secondary Data Source: Why Did International Adoption Suddenly End?
Despite a sharp decline in adoptions many SLPs still frequently continue to receive internationally adopted (IA) children for assessment as well as treatment – immediately post adoption as well as a number of years post-institutionalization.
In the age of social media, it may be very easy to pose questions and receive instantaneous responses on platforms such as Facebook and Twitter with respect to assessment and treatment recommendations. However, it is very important to understand that many SLPs, who lack direct clinical experience in international adoptions may chime in with inappropriate recommendations with respect to the assessment or treatment of these children.
Consequently, it is important to identify reputable sources of information when it comes to speech-language assessment of internationally adopted children.
There are a number of researchers in both US and abroad who specialize in speech-language abilities of Internationally Adopted children. This list includes (but is by far not limited to) the following authors:
- Boris Gindis
- Sharon Glennen
- Deborah Hwa-Froelich
- Kathleen A. Scott
- Jenny A. Roberts
- Karen E. Pollock
- M. Gay Masters
- Monica Dalen
The works of these researchers can be readily accessed in the ASHA Journals or via ResearchGate.
Meanwhile, here are some basic facts regarding internationally adopted children that all SLPs and parents need to know.
Demographics:
- A greater number of older, preschool and school-aged children and fewer number of infants and toddlers are placed for adoption (Selman, 2012).
- Significant increase in special needs adoptions from Eastern European countries (e.g., Ukraine, Kazhakstan, etc.) as well as China. The vast majority of Internationally Adopted children arrive to the United States with significant physical, linguistic, and cognitive disabilities as well as mental health problems. Consequently, it is important for schools to immediately provide the children with a host of services including speech-language therapy, immediately post-arrival.
- It is also important to know that in the vast majority of cases the child’s linguistic, cognitive, or mental health deficits may not be documented in the adoption records due to poor record keeping, lack of access to adequate healthcare or often to ensure their “adoptability”. As such, parental interviews and anecdotal evidence become the primary source of information regarding these children’s social and academic functioning in their respective birth countries.
The question of bilingualism:
- Internationally Adopted children are NOT bilingual children! In fact, the vast majority of internationally adopted children will very rapidly lose their birth language, in a period of 2-3 months post arrival (Gindis, 2005), since they are most often adopted by parents who do not speak the child’s birth language and as such are unable/unwilling to maintain it.
- IA children do not need to be placed in ESL classes since they are not bilingual children. Not only are IA children not bilingual, they are also not ‘truly’ monolingual since their first language is lost rather rapidly, while their second language has been gained minimally at the time of loss.
- IA children need to acquire Cognitive Language Mastery (CLM) which is language needed for formal academic learning. This includes listening, speaking, reading, and writing about subject area content material including analyzing, synthesizing, judging and evaluating presented information. This level of language learning is essential for a child to succeed in school. CLM takes years and years to master, especially because, IA children did not have the same foundation of knowledge and stimulation as bilingual children in their birth countries.

- IA children’s language abilities should be retested and monitored at regular intervals during the first several years post arrival.
- Glennen (2007) recommends 3 evaluations during the first year post arrival, with annual reevaluations thereafter.
- Hough & Kaczmarek (2011) recommend a reevaluation schedule of 3-4 times a year for a period of two years, post arrival because some IA children continue to present with language-based deficits many years (5+) post-adoption.
- If an SLP speaking the child’s first language is available the window of opportunity to assess in the first language is very limited (~2-3 months at most).
- Similarly, an assessment with an interpreter is recommended immediately post arrival from the birth country for a period of approximately the same time.
- If an SLP speaking the child’s first language is not available English-speaking SLP should consider assessing the child in English between 3-6 months post arrival (depending on the child and the situational constraints) in order to determine the speed with which s/he are acquiring English language abilities
- Children should be demonstrating rapid language gains in the areas of receptive language, vocabulary as well as articulation (Glennen 2007, 2009)
- Dynamic assessment is highly recommended
- It is important to remember that language and literacy deficits are not always very apparent and can manifest during any given period post arrival
To treat or NOT to Treat?
- “Any child with a known history of speech and language delays in the sending country should be considered to have true delays or disorders and should receive speech and language services after adoption.” (Glennen, 2009, p.52)
- IA children with medical diagnoses, which impact their speech language abilities should be assessed and considered for S-L therapy services as well (Ladage, 2009).
Helpful Links:
- Elleseff, T (2013) Changing Trends in International Adoption: Implications for Speech-Language Pathologists. Perspectives on Global Issues in Communication Sciences and Related Disorders, 3: 45-53
- Assessing Behaviorally Impaired Students: Why Background History Matters!
- Dear School Professionals Please Be Aware of This
- What parents need to know about speech-language assessment of older internationally adopted children
- Understanding the risks of social pragmatic deficits in post institutionalized internationally adopted (IA) children
- Understanding the extent of speech and language delays in older internationally adopted children
References:
- Gindis, B. (2005). Cognitive, language, and educational issues of children adopted from overseas orphanages. Journal of Cognitive Education and Psychology, 4 (3): 290-315.
- Glennen, S (2009) Speech and language guidelines for children adopted from abroad at older ages. Topics in language Disorders 29, 50-64.
- Ladage, J. S. (2009). Medical Issues in International Adoption and Their Influence on Language Development. Topics in Language Disorders , 29 (1), 6-17.
- Selman P. (2012) Global trends in Intercountry Adoption 2000-2010. New York: National Council for Adoption, 2012.
- Selman P. The global decline of intercountry adoption: What lies ahead?. Social Policy and Society 2012, 11(3), 381-397.
Additional Helpful References:
- Abrines, N., Barcons, N., Brun, C., Marre, D., Sartini, C., & Fumadó, V. (2012). Comparing ADHD symptom levels in children adopted from Eastern Europe and from other regions: discussing possible factors involved. Children and Youth Services Review, 34 (9) 1903-1908.
- Balachova, T et al (2010). Changing physicians’ knowledge, skills and attitudes to prevent FASD in Russia: 800. Alcoholism: Clinical & Experimental Research. 34(6) Sup 2:210A.
- Barcons-Castel, N, Fornieles-Deu,A, & Costas-Moragas, C (2011). International adoption: assessment of adaptive and maladaptive behavior of adopted minors in Spain. The Spanish Journal of Psychology, 14 (1): 123-132.
- Beverly, B., McGuinness, T., & Blanton, D. (2008). Communication challenges for children adopted from the former Soviet Union. Language, Speech, and Hearing Services in Schools, 39, 1-11.
- Cohen, N. & Barwick, M. (1996). Comorbidity of language and social-emotional disorders: comparison of psychiatric outpatients and their siblings. Journal of Clinical Child Psychology, 25(2), 192-200.
- Croft, C et al, (2007). Early adolescent outcomes of institutionally-deprived and nondeprived adoptees: II. Language as a protective factor and a vulnerable outcome. The Journal of Child Psychology and Psychiatry, 48, 31–44.
- Dalen, M. (2001). School performances among internationally adopted children in Norway. Adoption Quarterly, 5(2), 39-57.
- Dalen, M. (1995). Learning difficulties among inter-country adopted children. Nordisk pedagogikk, 15 (No. 4), 195-208
- Davies, J., & Bledsoe, J. (2005). Prenatal alcohol and drug exposures in adoption. Pediatric Clinics of North America, 52, 1369–1393.
- Desmarais, C., Roeber, B. J., Smith, M. E., & Pollak, S. D. (2012). Sentence comprehension in post-institutionalized school-age children. Journal of Speech, Language, and Hearing Research, 55, 45-54
- Eigsti, I. M., Weitzman, C., Schuh, J. M., de Marchena, A., & Casey, B. J. (2011). Language and cognitive outcomes in internationally adopted children. Development and Psychopathology, 23, 629-646.
- Geren, J., Snedeker, J., & Ax, L. (2005). Starting over: a preliminary study of early lexical and syntactic development in internationally-adopted preschoolers. Seminars in Speech & Language, 26:44-54.
- Gindis (2008) Abrupt native language loss in international adoptees. Advance for Speech/Language Pathologists and Audiologists. 18(51): 5.
- Gindis, B. (2005). Cognitive, language, and educational issues of children adopted from overseas orphanages. Journal of Cognitive Education and Psychology, 4 (3): 290-315. Gindis, B. (1999) Language-related issues for international adoptees and adoptive families. In: T. Tepper, L. Hannon, D. Sandstrom, Eds. “International Adoption: Challenges and Opportunities.” PNPIC, Meadow Lands , PA. , pp. 98-108
- Glennen, S (2009) Speech and language guidelines for children adopted from abroad at older ages. Topics in language Disorders 29, 50-64.
- Glennen, S. (2007) Speech and language in children adopted internationally at older ages. Perspectives on Communication Disorders in Culturally and Linguistically Diverse Populations, 14, 17–20.
- Glennen, S., & Bright, B. J. (2005). Five years later: language in school-age internally adopted children. Seminars in Speech and Language, 26, 86-101.
- Glennen, S. & Masters, G. (2002). Typical and atypical language development in infants and toddlers adopted from Eastern Europe. American Journal of Speech-Language Pathology, 44, 417-433
- Gordina, A (2009) Parent Handout: The Dream Referral, Unpublished Manuscript.
- Hough, S., & Kaczmarek, L. (2011). Language and reading outcomes in young children adopted from Eastern European orphanages. Journal of Early Intervention, 33, 51-57.
- Hwa-Froelich, D (2012) Childhood maltreatment and communication development. Perspectives on School-Based Issues, 13: 43-53;
- Jacobs, E., Miller, L. C., & Tirella, G. (2010). Developmental and behavioral performance of internationally adopted preschoolers: a pilot study. Child Psychiatry and Human Development, 41, 15–29.
- Jenista, J., & Chapman, D. (1987). Medical problems of foreign-born adopted children. American Journal of Diseases of Children, 141, 298–302.
- Johnson, D. (2000). Long-term medical issues in international adoptees. Pediatric Annals, 29, 234–241.
- Judge, S. (2003). Developmental recovery and deficit in children adopted from Eastern European orphanages. Child Psychiatry and Human Development, 34, 49–62.
- Krakow, R. A., & Roberts, J. (2003). Acquisitions of English vocabulary by young Chinese adoptees. Journal of Multilingual Communication Disorders, 1, 169-176
- Ladage, J. S. (2009). Medical issues in international adoption and their influence on language development. Topics in Language Disorders , 29 (1), 6-17.
- Loman, M. M., Wiik, K. L., Frenn, K. A., Pollak, S. D., & Gunnar, M. R. (2009). Post-institutionalized children’s development: growth, cognitive, and language outcomes. Journal of Developmental Behavioral Pediatrics, 30, 426–434.
- McLaughlin, B., Gesi Blanchard, A., & Osanai, Y. (1995). Assessing language development in bilingual preschool children. Washington, D.C.: National Clearinghouse for Bilingual Education.
- Miller, L., Chan, W., Litvinova, A., Rubin, A., Tirella, L., & Cermak, S. (2007). Medical diagnoses and growth of children residing in Russian orphanages. Acta Paediatrica, 96, 1765–1769.
- Miller, L., Chan, W., Litvinova, A., Rubin, A., Comfort, K., Tirella, L., et al. (2006). Fetal alcohol spectrum disorders in children residing in Russian orphanages: A phenotypic survey. Alcoholism: Clinical and Experimental Research, 30, 531–538.
- Miller, L. (2005). Preadoption counseling and evaluation of the referral. In L. Miller (Ed.), The Handbook of International Adoption Medicine (pp. 67-86). NewYork: Oxford.
- Pollock, K. E. (2005) Early language growth in children adopted from China: preliminary normative data. Seminars in Speech and Language, 26, 22-32.
- Roberts, J., Pollock, K., Krakow, R., Price, J., Fulmer, K., & Wang, P. (2005). Language development in preschool-aged children adopted from China. Journal of Speech, Language, and Hearing Research, 48, 93–107.
- Scott, K.A., Roberts, J.A., & Glennen, S. (2011). How well children who are internationally do adopted acquire language? A meta-analysis. Journal of Speech, Language and Hearing Research, 54. 1153-69.
- Scott, K.A., & Roberts, J. (2011). Making evidence-based decisions for children who are internationally adopted. Evidence-Based Practice Briefs. 6(3), 1-16.
- Scott, K.A., & Roberts, J. (2007) language development of internationally adopted children: the school-age years. Perspectives on Communication Disorders in Culturally and Linguistically Diverse Populations, 14: 12-17.
- Selman P. (2012a) Global trends in intercountry adoption 2000-2010. New York: National Council for Adoption.
- Selman P (2012b). The rise and fall of intercountry adoption in the 21st century. In: Gibbons, J.L., Rotabi, K.S, ed. Intercountry Adoption: Policies, Practices and Outcomes. London: Ashgate Press.
- Selman, P. (2010) “Intercountry adoption in Europe 1998–2009: patterns, trends and issues,” Adoption & Fostering, 34 (1): 4-19.
- Silliman, E. R., & Scott, C. M. (2009). Research-based oral language intervention routes to the academic language of literacy: Finding the right road. In S. A. Rosenfield & V. Wise Berninger (Eds.), Implementing evidence-based academic interventions in school (pp. 107–145). New York: Oxford University Press.
- Tarullo, A. R., Bruce, J., & Gunnar, M. (2007). False belief and emotion understanding in post-institutionalized children. Social Development, 16, 57-78
- Tarullo, A. & Gunnar, M. R. (2005). Institutional rearing and deficits in social relatedness: Possible mechanisms and processes. Cognitie, Creier, Comportament [Cognition, Brain, Behavior], 9, 329-342.
- Varavikova, E. A. & Balachova, T. N. (2010). Strategies to implement physician training in FAS prevention as a part of preventive care in primary health settings: P120.Alcoholism: Clinical & Experimental Research. 34(8) Sup 3:119A.
- Welsh, J. A., & Viana, A. G. (2012). Developmental outcomes of children adopted internationally. Adoption Quarterly, 15, 241-264.
Assessing Behaviorally Impaired Students: Why Background History Matters!
 As a speech language pathologist (SLP) who works in an outpatient psychiatric school-based setting, I frequently review incoming students previous speech language evaluation reports. There are a number of trends I see in these reports which I have written about in the past as well as planned on writing about in the future.
As a speech language pathologist (SLP) who works in an outpatient psychiatric school-based setting, I frequently review incoming students previous speech language evaluation reports. There are a number of trends I see in these reports which I have written about in the past as well as planned on writing about in the future.
For example, in the past I wrote about my concern regarding the lack of adequate or even cursory social communication assessments for students with documented psychiatric impairments and emotional behavioral deficits.
This leads many professionals to do the following:
a. Miss vital assessment elements which denies students appropriate school based services and
b. Assume that the displayed behavioral challenges are mere results of misbehaving.
Today however I wanted express my thoughts regarding another disturbing trend I see in numerous incoming speech-language reports in both outpatient school/hospital setting as well as in private practice – and that is lack of background information in the students assessment reports.
Despite its key role in assessment, this section is frequently left bare. Most of the time it contains only the information regarding the students age and grade levels as well as the reasons for the referral (e.g., initial evaluation, triennial evaluation). Some of the better reports will include cursory mention of the student’s developmental milestones but most of the time information will be sorely lacking.
Clearly this problem is not just prevalent in my incoming assessment reports. I frequently see manifestations of it in a variety of speech pathology related social media forums such as Facebook. Someone will pose a question regarding how to distinguish a _____ from ____ (e.g., language difference vs. language disorder, behavioral noncompliance vs. social communication deficits, etc.) yet when they’re questioned further many SLPs will admit that they are lacking any/most information regarding the students background history.
When questioned regarding the lack of this information, many SLPs get defensive. They cite a variety of reasons such as lack of parental involvement (“I can’t reach the parents”), lack of access to records (“it’s a privacy issue”), division of labor (e.g., “it’s the social worker’s responsibility and not mine to obtain this information”) as well as other justifications why this information is lacking.

Now, I don’t know about you, but one of my earliest memories of the ‘diagnostics’ class in graduate school involved collecting data and writing comprehensive ‘Background Information’ section of the report. I still remember multiple professors imparting upon me the vital importance is this section plays in the student’s evaluation report.
Indeed, many years later, I clearly see its vital role in assessment. Unearthing the student’s family history, developmental milestones, medical/surgical history, as well as history of past therapies is frequently the key to a successful diagnosis and appropriate provision of therapy services. This is the information that frequently plays a vital role in subsequent referrals of “mystery” cases to relevant health professionals as well as often leads to resolution of particularly complicated diagnostic puzzles.
Of course I understand that frequently there are legitimate barriers to obtaining this information. However, I also know that if one digs deep enough one will frequently find the information they’re seeking despite the barriers. To illustrate, at the psychiatric hospital level where I work, I frequently encounter a number of barriers to accessing the student’s background information during the assessment process. This may include parental language/education barrier, parental absence, Division of Child Protective Services involvement, etc. Yet I always try to ensure that my reports contain all the background information that I’m able to unearth because I know how vitally important it is for the student in question.
In the past I have been able to use the student’s background information to make important discoveries, which were otherwise missed by other health professionals. This included undocumented history of traumatic brain injuries, history of language and literacy disabilities in the family, history of genetic disorders and/or intellectual disabilities in the family, history of maternal alcohol abuse during pregnancy, and much much more.
So what do I consider to be an adequate Background History section of the assessment report?
For starters, the basics, of course.
I begin by stating the child’s age and grade levels, who referred the child (and for what reason), as well as whether the child previously received any form of speech language assessment/therapy services in the past.
If I am preforming a reassessment (especially if it happens shortly after the last assessment took place) I provide a clear justification why the present reassessment is taking place. Here is an actual excerpt from one of my reevaluation reports. “Despite receiving average language scores on his _______ speech language testing which resulted in the recommendation for speech therapy only, upon his admission to ______, student was referred for a language reassessment in _____, by the classroom staff who expressed significant concerns regarding validity and reliability of past speech and language testing on the ground of the student’s persistent “obvious” listening comprehension and verbal expression deficits.”
For those of you in need of further justification I’ve created a brief list of reasons why a reassessment, closely following recent testing may be needed.
- SLP/Parent feels additional testing is needed to create comprehensive goals for child.
- Previous testing was inadequate. Here it’s very important to provide comprehensive rationale and list the reasons for it.
- A reevaluation was requested due to third party concerns (e.g., psychiatrist, psychologist, etc.)
Secondly, it is important to document all relevant medical history, which includes: prenatal, perinatal, and early childhood diseases, surgical interventions and incidents. It is important to note that if a child has a long standing history of documented psychiatric difficulties, you may want to separate these sections and describe psychiatric history/diagnoses following the section that details the onset of the child’s emotional and behavioral deficits.

Let us now move on to the child’s developmental history, which should include, gross/fine motor, speech/ language milestones, and well as cognitive and socioemotional functioning. This is a section where I typically add information regarding any early intervention services which may have been provided to the child prior to the age of three.
In my next section I discuss the child’s academic functioning to date. Here I mention whether the student qualified for a preschool disabled eligibility category and received services from the age of 3+. I also discuss their educational classification (if one exists), briefly mention the results of previous most recent cognitive and educational testing (if available) as well as mention any academic struggles (if applicable).
After that I move on to the child’s psychiatric history. I briefly document when did the emotional behavioral problems first arose, and what had been done about them to date (out of district placements, variety of psychiatric services, etc.) Here I also document the student’s most recent psychiatric diagnoses (if available) and mention any medication they may be currently on (applicable due to the effect of psychiatric medications on language and memory skills).
The following section is perhaps the most important one in the report. It is the family’s history of genetic disorders, psychiatric impairments, special education placements, as well as language, learning, and literacy deficits. This section plays a vital importance in my determination of the contributions to the student’s language difficulties as well as guides my assessment recommendations in the presence of borderline assessment results.
I finish this section by briefly discussing the student’s Family Composition as well as Language Knowledge and Use.
I discuss family composition due to several factors. For example, lack of consistent caregivers, prolonged absence of parental figures, as well as presence of a variety of people in the home can serve as significant stressor for children with psychiatric impairments and learning difficulties. As a result of this information is pertinent to the report especially when it comes to figuring out the antecedents for the child’s behavior fluctuation on daily basis.

Language knowledge and use is particularly relevant to culturally and linguistically diverse children. It is very important to understand what languages does the child understand and use at home and at school as well as what do the parents think about the child’s language abilities in both languages. These factors will guide my decision making process regarding what type of assessments would be most relevant for this child.
So there you have it. This is the information I include in the background history section of every single one of my reports. I believe that this information contributes to the making of the appropriate and accurate diagnosis of the child’s difficulties.
Please don’t get me wrong. This information is hugely relevant for all students that we SLPs are assessing.
However, the above is especially relevant for such vulnerable populations as children with emotional and behavioral disturbances, whose struggle with social communication is frequently misinterpreted as “it’s just behavior“. As a result, they are frequently denied social communication therapy services, which ultimately leads to denial of Free Appropriate Public Education (FAPE) that they are entitled to.
Let us ensure that this does not happen by doing all that we can to endure that the student receives a fair assessment, correct diagnosis, and can have access to the best classroom placement, appropriate accommodations and modifications as well as targeted and relevant therapeutic services. And the first step of that process begins with obtaining a detailed background history!
Helpful Resources:
- Pediatric History Questionnaire
- The Checklists Bundle
- Introduction to Social Pragmatic Language Disorders
- Recognizing the Warning Signs of Social Emotional Difficulties in Language Impaired Toddlers and Preschoolers
- Social Pragmatic Deficits Checklist for Preschool Children
- Social Pragmatic Deficits Checklist for School Aged Children
- Social Pragmatic Assessment and Treatment Bundle
- Narrative Assessment Bundle
- Psychiatric Disorders Bundle
- Fetal Alcohol Spectrum Disorders Assessment and Treatment Bundle
- Assessing Social Pragmatic Skills of School Aged Children
- Behavior Management Strategies for Speech Language Pathologists
- Effective Behavior Management Techniques for Parents and Professionals
- Treatment of Social Pragmatic Deficits in School Aged Children
- Social Pragmatic Language Activity Pack
- Social Pragmatic Language: Multiple Interpretations Therapy Activity
- The Role of Frontal Lobe in Speech and Language Functions
- Executive Function Impairments in At-Risk Pediatric Populations
- Differential Diagnosis of ADHD in Speech Language Pathology
- Speech Language Assessment of Older Internationally Adopted Children
- General Assessment and Treatment Start Up Bundle
- Multicultural Assessment Bundle
Parent Consultation Services
 Today I’d like to officially introduce a new parent consultation service which I had originally initiated with a few out-of-state clients through my practice a few years ago.
Today I’d like to officially introduce a new parent consultation service which I had originally initiated with a few out-of-state clients through my practice a few years ago.
The idea for this service came after numerous parents contacted me and initiated dialogue via email and phone calls regarding the services/assessments needed for their monolingual/bilingual internationally/domestically adopted or biological children with complex communication needs. Here are some details about it.
Parent consultations is a service provided to clients who live outside Smart Speech Therapy LLC geographical area (e.g., non-new Jersey residents) who are interested in comprehensive specialized in-depth consultations and recommendations regarding what type of follow up speech language services they should be seeking/obtaining in their own geographical area for their children as well as what type of carryover activities they should be doing with their children at home.
Consultations are provided with the focus on the following specialization areas with a focus on comprehensive assessment and intervention recommendations:
- Language and Literacy
- Children with Social Communication (Pragmatic) Disorders
- Bilingual and Multicultural Children
- Post-institutionalized Internationally Adopted Children
- Children with Psychiatric and Emotional Disturbances
- Children with Fetal Alcohol Spectrum Disorders
The initial consultation length of this service is 1 hour. Clients are asked to forward their child’s records prior to the consultation for review, fill out several relevant intakes and questionnaires, as well as record a short video (3-5 minutes). The instructions regarding video content will be provided to them following session payment.
Upon purchasing a consultation the client will be immediately emailed the necessary paperwork to fill out as well as potential dates and times for the consultation to take place. Afternoon, Evening and Weekend hours are available for the client’s convenience. In cases of emergencies consultations may be rescheduled at the client’s/Smart Speech Therapy’s mutual convenience.
Refunds are available during a 3 day grace period if a mutually convenient time could not be selected for the consultation. Please note that fees will not be refundable from the time the scheduled consultation begins.
Following the consultation the client has the option of requesting a written detailed consultation report at an additional cost, which is determined based on the therapist’s hourly rate. For further information click HERE. You can also call 917-916-7487 or email tatyana.elleseff@smartspeechtherapy.com if you wanted to find out whether this service is right for you.
Below is a past parent consultation testimonial.
International Adoption Consultation Parent Testimonial (11/11/13)
I found Tatyana and Smart Speech Therapy online while searching for information about internationally adopted kids and speech evaluations. We’d already taken our three year old son to a local SLP but were very unsatisfied with her opinion, and we just didn’t know where to turn. Upon finding the articles and blogs written by Tatyana, I felt like I’d finally found someone who understood the language learning process unique to adopted kids, and whose writings could also help me in my meetings with the local school system as I sought special education services for my son.
I could have never predicted then just how much Tatyana and Smart Speech Therapy would help us. I used the online contact form on her website to see if Tatyana could offer us any services or recommendations, even though we are in Virginia and far outside her typical service area. She offered us an in-depth phone consultation that was probably one of the most informative, supportive and helpful phone calls I’ve had in the eight months since adopting my son. Through a series of videos, questionnaires, and emails, she was better able to understand my son’s speech difficulties and background than any of the other sources I’d sought help from. She was able to explain to me, a lay person, exactly what was going on with our son’s speech, comprehension, and learning difficulties in a way that a) added urgency to our situation without causing us to panic, b) provided me with a ton of research-orientated information for our local school system to review, and c) validated all my concerns and gut instincts that had previously been brushed aside by other physicians and professionals who kept telling us to “wait and see”.
After our phone call, we contracted Tatyana to provide us with an in-depth consultation report that we are now using with our local school and child rehab center to get our son the help he needs. Without that report, I don’t think we would have had the access to these services or the backing we needed to get people to seriously listen to us. It’s a terrible place to be in when you think something might be wrong, but you’re not sure and no one around you is listening. Tatyana listened to us, but more importantly, she looked at our son as a specific kid with a specific past and specific needs. We were more than just a number or file to her – and we’ve never even actually met in person! The best move we’ve could’ve made was sending her that email that day. We are so appreciative.
Kristen, P. Charlottesville, VA
Assessing Social Communication Abilities of School-Aged Children
 Recently, I’ve published an article in SIG 16 Perspectives on School Based Issues discussing the importance of social communication assessments of school aged children 2-18 years of age. Below I would like to summarize article highlights.
Recently, I’ve published an article in SIG 16 Perspectives on School Based Issues discussing the importance of social communication assessments of school aged children 2-18 years of age. Below I would like to summarize article highlights.
First, I summarize the effect of social communication on academic abilities and review the notion of the “academic impact”. Then, I go over important changes in terminology and definitions as well as explain the “anatomy of social communication”.
Next I suggest a sample social communication skill hierarchy to adequately determine assessment needs (assess only those abilities suspected of deficits and exclude the skills the student has already mastered).
After that I go over pre-assessment considerations as well as review standardized testing and its limitations from 3-18 years of age.
Finally I review a host of informal social communication procedures and address their utility.
What is the away message?
When evaluating social communication, clinicians need to use multiple assessment tasks to create a balanced assessment. We need to chose testing instruments that will help us formulate clear goals. We also need to add descriptive portions to our reports in order to “personalize” the student’s deficit areas. Our assessments need to be functional and meaningful for the student. This means determining the student’s strengths and not just weaknesses as a starting point of intervention initiation.
Is this an article which you might find interesting? If so, you can access full article HERE free of charge.
Helpful Smart Speech Resources Related to Assessment and Treatment of Social Communication
- Gauging Moods and Interpreting Emotional States
- Social Pragmatic Language Activity Pack
- Social Pragmatic Language: Multiple Interpretations Therapy Activity
- Social Pragmatic Photo Bundle for Early Elementary Aged Children
- Introduction to Social Pragmatic Language Disorders
- Recognizing the Warning Signs of Social Emotional Difficulties in Language Impaired Toddlers and Preschoolers
- Social Pragmatic Deficits Checklist for Preschool Children
- Social Pragmatic Deficits Checklist for School Aged Children
- Social Pragmatic Assessment and Treatment Bundle
- Narrative Assessment Bundle
- Psychiatric Disorders Bundle
- Fetal Alcohol Spectrum Disorders Assessment and Treatment Bundle
- Assessing Social Pragmatic Skills of School Aged Children
- Behavior Management Strategies for Speech Language Pathologists
- Effective Behavior Management Techniques for Parents and Professionals
- Assessment and Treatment of Non-Verbal Language Disorder (NVLD) in Speech Language Pathology
- Treatment of Social Pragmatic Deficits in School Aged Children
- The Role of Frontal Lobe in Speech and Language Functions
- Executive Function Impairments in At-Risk Pediatric Populations
- Differential Diagnosis of ADHD in Speech Language Pathology
- Speech Language Assessment of Older Internationally Adopted Children
- ABBN0002: Early Identification of Language-Based Deficits in Pediatric Populations [Recorded CEU Webinar]