 So you’ve completed a thorough evaluation of your student’s speech and language abilities and are in the process of creating goals and objectives to target in sessions. The problem is that many of the students on our caseloads present with pervasive deficits in many areas of language.
So you’ve completed a thorough evaluation of your student’s speech and language abilities and are in the process of creating goals and objectives to target in sessions. The problem is that many of the students on our caseloads present with pervasive deficits in many areas of language.
While it’s perfectly acceptable to target just a few goals per session in order to collect good data, both research and clinical experience indicate that addressing goals comprehensively and thematically (the whole system or multiple goals at once from the areas of content, form, and use) via contextual language intervention vs. in isolation (small parts such as prepositions, pronouns, etc.) will bring about the quickest change and more permanent results.

So how can that be done? Well, for significantly language impaired students it’s very important to integrate semantic language components as well as verbal reasoning tasks into sessions no matter what type of language activity you are working on (such as listening comprehension, auditory processing, social inferencing and so on). The important part is to make sure that the complexity of the task is commensurate with the student’s level of abilities.

Let’s say you are working on a fall themed lesson plans which include topics such as apples and pumpkins. As you are working on targeting different language goals, just throw in a few extra components to the session and ask the child to make, produce, explain, list, describe, identify, or interpret:
- Associations (“We just read a book about pumpkin: What goes with a pumpkin?”)
- Synonyms (“It said the leaves felt rough, what’s another word for rough?”)
- Antonyms (“what is the opposite of rough?”)
- Attributes 5+ (category, function, location, appearance, accessory/necessity, composition) (“Pretend I don’t know what a pumpkin is, tell me everything you can think of about a pumpkin”)
- Multiple Meaning Words (“The word felt has two meanings, it could mean _____ and it could also mean _______”)
- Definitions (“what is a pumpkin”)
- Compare and Contrast (“How are pumpkin and apple alike? How are they different?”)
- Idiomatic expressions (“Do you know what the phrase turn into a pumpkin means?” )
Ask ‘why’ and ‘how’ questions in order to start teaching the student how to justify, rationalize, evaluate, and make judgments regarding presented information (“Why do you think we plant pumpkins in the spring and not in the fall?”)
Don’t forget the inferencing and predicting questions in order to further develop the client’s verbal reasoning abilities (“What do you think will happen if no one picks up the apples from the ground?)
If possible attempt to integrate components of social language into the session such as ask client to relate to a character in a story, interpret the character’s feelings (“How do you think the girl felt when her sisters made fun of her pumpkin?”), ideas and thoughts, or just read nonverbal social cues such as body language or facial expressions of characters in pictures.
Select materials which are both multipurpose and reusable as well as applicable to a variety of therapy goals. For example, let’s take a simple seasonal word wall such as the (free) Fall Word Wall from TPT by Pocketful of Centers. Print it out in color, cut out the word strips and note how many therapy activities you can target for articulation, language, fluency, literacy and phonological awareness, etc.

Language:
Practice Categorization skills via convergent and divergent naming activities: Name Fall words, Name Halloween/Thanksgiving Words, How many trees whose leaves change color can you name?, how many vegetables and fruits do we harvest in the fall? etc.
Practice naming Associations: what goes with a witch (broom), what goes with a squirrel (acorn), etc
Practice providing Attributes via naming category, function, location, parts, size, shape, color, composition, as well as accessory/necessity. For example, (I see a pumpkin. It’s a fruit/vegetable that you can plant, grow and eat. You find it on a farm. It’s round and orange and is the size of a ball. Inside the pumpkin are seeds. You can carve it and make a jack o lantern out of it).
Practice providing Definitions: Tell me what a skeleton is. Tell me what a scarecrow is.
Practice naming Similarities and Differences among semantically related items: How are pumpkin and apple alike? How are they different?
Practice explaining Multiple Meaning words: What are some meanings of the word bat, witch, clown, etc?
Practice Complex Sentence Formulation: what happens in the fall? Make up a sentence with the words scarecrow and unless, make up a sentence with the words skeleton and however, etc

Phonological Awareness:
Practice Rhyming words (you can do discrimination and production activities): cat/bat/ trick/leaf/ rake/moon
Practice Syllable and Phoneme Segmentation (I am going to say a word (e.g., leaf, corn, scarecrow, etc) and I want you to clap one time for each syllable or sound I say)
Practice Isolation of initial, medial, and final phonemes in words ( e.g., What is the beginning/final sound in apple, hay, pumpkin etc?) What is the middle sound in rake etc?
Practice Initial and Final Syllable and Phoneme Deletion in Words (Say spider! Now say it without the der, what do you have left? Say witch, now say it without the /ch/ what is left; say corn, now say it without the /n/, what is left?)
Articulation/Fluency:
Practice production of select sounds/consonant clusters that you are working on or just production at word or sentence levels with those clients who just need a little bit more work in therapy increasing their intelligibility or sentence fluency.
So next time you are targeting your goals, see how you can integrate some of these suggestions into your data collection and let me know whether or not you’ve felt that it has enhanced your therapy sessions.
Happy Speeching! 
Helpful Resources:
- Creating Functional Therapy Plan
- Selecting Clinical Materials for Pediatric Therapy
- Vocabulary Development: Working With Disadvantaged Populations
- General Assessment and Treatment Start-Up Bundle

 September is practically here and many speech language pathologists (SLPs) are looking to efficiently prepare for assessing and treating a variety of clients on their caseloads.
September is practically here and many speech language pathologists (SLPs) are looking to efficiently prepare for assessing and treating a variety of clients on their caseloads.
 Today I am writing my last installment in the five-part early intervention assessment series. My
Today I am writing my last installment in the five-part early intervention assessment series. My 
 Spoon Stripping and Mouth Closure: During the yogurt presentation, AK’s spoon stripping abilities and mouth closure were deemed good (adequate) when fed by a caregiver and fair when AK fed self (incomplete food stripping from the spoon was observed due to only partial mouth closure). According to parental report, AK’s spoon stripping abilities have improved in recent months. Ms. K was observed to present spoon upwardly in AK’s mouth and hold it still until AK placed her lips firmly around the spoon and initiated spoon stripping. Since this strategy is working adequately for all parties in question no further recommendations regarding spoon feeding are necessary at this time. Skill monitoring is recommended on an ongoing basis for further refinement.
Spoon Stripping and Mouth Closure: During the yogurt presentation, AK’s spoon stripping abilities and mouth closure were deemed good (adequate) when fed by a caregiver and fair when AK fed self (incomplete food stripping from the spoon was observed due to only partial mouth closure). According to parental report, AK’s spoon stripping abilities have improved in recent months. Ms. K was observed to present spoon upwardly in AK’s mouth and hold it still until AK placed her lips firmly around the spoon and initiated spoon stripping. Since this strategy is working adequately for all parties in question no further recommendations regarding spoon feeding are necessary at this time. Skill monitoring is recommended on an ongoing basis for further refinement.  Cup and Straw Drinking: AK was also observed to drink 40 mls of water from a cup given parental assistance. Minor anterior spillage was intermittently noted during liquid intake. It is recommended that the parents modify cup presentation by providing AK with a plastic cup with two handles on each side, which would improve her ability to grasp and maintain hold on cup while drinking.
Cup and Straw Drinking: AK was also observed to drink 40 mls of water from a cup given parental assistance. Minor anterior spillage was intermittently noted during liquid intake. It is recommended that the parents modify cup presentation by providing AK with a plastic cup with two handles on each side, which would improve her ability to grasp and maintain hold on cup while drinking. In the past several years, due to an influx of adolescent students with language and learning difficulties on my caseload, I have begun to research in depth aspects of adolescent
In the past several years, due to an influx of adolescent students with language and learning difficulties on my caseload, I have begun to research in depth aspects of adolescent  For this purpose, I often use the books from the Continental Press series entitled:
For this purpose, I often use the books from the Continental Press series entitled: 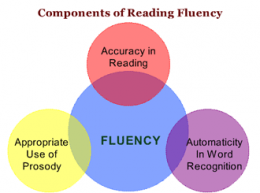 Reading Fluency: TS’s reading fluency (automaticity, prosody, accuracy and speed, expression, intonation, and phrasing) during the reading task was marked by monotone vocal quality, awkward word stress, imprecise articulatory contacts, false-starts, self–revisions, awkward mid-sentential pauses, limited pausing for punctuation, as well as misreadings and word substitutions, all of which resulted in an impaired reading prosody.
Reading Fluency: TS’s reading fluency (automaticity, prosody, accuracy and speed, expression, intonation, and phrasing) during the reading task was marked by monotone vocal quality, awkward word stress, imprecise articulatory contacts, false-starts, self–revisions, awkward mid-sentential pauses, limited pausing for punctuation, as well as misreadings and word substitutions, all of which resulted in an impaired reading prosody. Text Vocabulary Comprehension:
Text Vocabulary Comprehension: Impressions: Clinical below grade-level reading comprehension assessment reading revealed that TS presents with a number of reading related difficulties. TS’s reading fluency was marked by monotone vocal quality, awkward word stress, imprecise articulatory contacts, false-starts, self–revisions, awkward mid-sentential pauses, limited pausing for punctuation, as well as misreadings and word substitutions, all of which resulted in an impaired reading prosody. TS’s understanding as well as his verbal summary of the presented text was immature for his age and was characterized by impaired gestalt processing of information resulting in an ineffective and confusing summarization. While TS’s text-based vocabulary knowledge was deemed to be grossly adequate for his age, his reading comprehension abilities were judged to be impaired for his age. Therapeutic intervention is strongly recommended to improve TS’s reading abilities. (See Impressions and Recommendations sections for further details).
Impressions: Clinical below grade-level reading comprehension assessment reading revealed that TS presents with a number of reading related difficulties. TS’s reading fluency was marked by monotone vocal quality, awkward word stress, imprecise articulatory contacts, false-starts, self–revisions, awkward mid-sentential pauses, limited pausing for punctuation, as well as misreadings and word substitutions, all of which resulted in an impaired reading prosody. TS’s understanding as well as his verbal summary of the presented text was immature for his age and was characterized by impaired gestalt processing of information resulting in an ineffective and confusing summarization. While TS’s text-based vocabulary knowledge was deemed to be grossly adequate for his age, his reading comprehension abilities were judged to be impaired for his age. Therapeutic intervention is strongly recommended to improve TS’s reading abilities. (See Impressions and Recommendations sections for further details). As SLPs we routinely administer a variety of testing batteries in order to assess our students’ speech-language abilities. Grammar, syntax, vocabulary, and sentence formulation get frequent and thorough attention. But how about narrative production? Does it get its fair share of attention when the clinicians are looking to determine the extent of the child’s language deficits? I was so curious about what the clinicians across the country were doing that in 2013, I created a survey and posted a link to it in several SLP-related FB groups. I wanted to find out how many SLPs were performing narrative assessments, in which settings, and with which populations. From those who were performing these assessments, I wanted to know what type of assessments were they using and how they were recording and documenting their findings. Since the purpose of this survey was non-research based (I wasn’t planning on submitting a research manuscript with my findings), I only analyzed the first 100 responses (the rest were very similar in nature) which came my way, in order to get the general flavor of current trends among clinicians, when it came to narrative assessments. Here’s a brief overview of my [limited] findings.
As SLPs we routinely administer a variety of testing batteries in order to assess our students’ speech-language abilities. Grammar, syntax, vocabulary, and sentence formulation get frequent and thorough attention. But how about narrative production? Does it get its fair share of attention when the clinicians are looking to determine the extent of the child’s language deficits? I was so curious about what the clinicians across the country were doing that in 2013, I created a survey and posted a link to it in several SLP-related FB groups. I wanted to find out how many SLPs were performing narrative assessments, in which settings, and with which populations. From those who were performing these assessments, I wanted to know what type of assessments were they using and how they were recording and documenting their findings. Since the purpose of this survey was non-research based (I wasn’t planning on submitting a research manuscript with my findings), I only analyzed the first 100 responses (the rest were very similar in nature) which came my way, in order to get the general flavor of current trends among clinicians, when it came to narrative assessments. Here’s a brief overview of my [limited] findings.  To date, I have written 3 posts on speech and language assessments of children under 3 years of age. My first post offered suggestions on what information to include in
To date, I have written 3 posts on speech and language assessments of children under 3 years of age. My first post offered suggestions on what information to include in 




 If I happen to know that a child is highly verbal, I may actually include a
If I happen to know that a child is highly verbal, I may actually include a  To illustrate, below is a narrative sample from a typically developing 2-year-old child based on the Mercer Mayer’s classic wordless picture book: “Frog Where Are You?”
To illustrate, below is a narrative sample from a typically developing 2-year-old child based on the Mercer Mayer’s classic wordless picture book: “Frog Where Are You?” Of course, a play assessment for this age group is a must. Since, in my first post,
Of course, a play assessment for this age group is a must. Since, in my first post,  For toddlers 18+months of age, I like using the Language Use Inventory (LUI)
For toddlers 18+months of age, I like using the Language Use Inventory (LUI)  In addition to the LUI, I recently discovered the
In addition to the LUI, I recently discovered the 




 In this post, I am continuing my series of articles on speech and language assessments of children under 3 years of age. My first installment in this series offered suggestions regarding what information to include in
In this post, I am continuing my series of articles on speech and language assessments of children under 3 years of age. My first installment in this series offered suggestions regarding what information to include in  As mentioned in my previous post on
As mentioned in my previous post on  Developmental Milestones expected of a 16-18 months old toddler:
Developmental Milestones expected of a 16-18 months old toddler:  Materials to use with the child to promote language and play:
Materials to use with the child to promote language and play:  Core vocabulary categories for listening and speaking:
Core vocabulary categories for listening and speaking: Summer is in full swing and for many SLPs that means a welcome break from work. However, for me, it’s business as usual, since my program is year around, and we have just started our extended school year program.
Summer is in full swing and for many SLPs that means a welcome break from work. However, for me, it’s business as usual, since my program is year around, and we have just started our extended school year program.

 After the completion of the screening, the app generates a two-page report which describes the students’ abilities as:
After the completion of the screening, the app generates a two-page report which describes the students’ abilities as: The Profile of Phonological Awareness (Pro-PA), an informal phonological awareness screening was administered to “Justine” in May 2017 to further determine the extent of her phonological awareness strengths and weaknesses.
The Profile of Phonological Awareness (Pro-PA), an informal phonological awareness screening was administered to “Justine” in May 2017 to further determine the extent of her phonological awareness strengths and weaknesses.