Writing! The one assessment area that challenges many SLPs on daily basis! If one polls 10 SLPs on the topic of writing, one will get 10 completely different responses ranging from agreement and rejection to the diverse opinions regarding what should actually be assessed and how exactly it should be accomplished.
Consequently, today I wanted to focus on the basics involved in the assessment of adolescent writing. Why adolescents you may ask? Well, frankly because many SLPs (myself included) are far more likely to assess the writing abilities of adolescents rather than elementary-aged children.
Often, when the students are younger and their literacy abilities are weaker, the SLPs may not get to the assessment of writing abilities due to the students presenting with so many other deficits which require precedence intervention-wise. However, as the students get older and the academic requirements increase exponentially, SLPs may be more frequently asked to assess the students’ writing abilities because difficulties in this area significantly affect them in a variety of classes on a variety of subjects.
So what can we assess when it comes to writing? In the words of Helen Lester’s character ‘Pookins’: “Lots!” There are various types of writing that can be assessed, the most common of which include: expository, persuasive, and fictional. Each of these can be used for assessment purposes in a variety of ways.
To illustrate, if we chose to analyze the student’s written production of fictional narratives then we may broadly choose to analyze the following aspects of the student’s writing: contextual conventions and writing composition.
 The former looks at such writing aspects as the use of correct spelling, punctuation, and capitalization, paragraph formation, etc.
The former looks at such writing aspects as the use of correct spelling, punctuation, and capitalization, paragraph formation, etc.
The latter looks at the nitty-gritty elements involved in plot development. These include effective use of literate vocabulary, plotline twists, character development, use of dialogue, etc.
Perhaps we want to analyze the student’s persuasive writing abilities. After all, high school students are expected to utilize this type of writing frequently for essay writing purposes. Actually, persuasive writing is a complex genre which is particularly difficult for students with language-learning difficulties who struggle to produce essays that are clear, logical, convincing, appropriately sequenced, and take into consideration opposing points of view. It is exactly for that reason that persuasive writing tasks are perfect for assessment purposes.
But what exactly are we looking for analysis wise? What should a typical 15 year old’s persuasive essays contain?
 With respect to syntax, a typical student that age is expected to write complex sentences possessing nominal, adverbial, as well as relative clauses.
With respect to syntax, a typical student that age is expected to write complex sentences possessing nominal, adverbial, as well as relative clauses.
With the respect to semantics, effective persuasive essays require the use of literate vocabulary words of low frequency such as later developing connectors (e.g., first of all, next, for this reason, on the other hand, consequently, finally, in conclusion) as well as metalinguistic and metacognitive verbs (“metaverbs”) that refer to acts of speaking (e.g., assert, concede, predict, argue, imply) and thinking (e.g., hypothesize, remember, doubt, assume, infer).
With respect to pragmatics, as students mature, their sensitivity to the perspectives of others improves, as a result, their persuasive essays increase in length (i.e., total number of words produced) and they are able to offer a greater number of different reasons to support their own opinions (Nippold, Ward-Lonergan, & Fanning, 2005).
Now let’s apply our knowledge by analyzing a writing sample of a 15-year-old with suspected literacy deficits. Below 10th-grade student was provided with a written prompt first described in the Nippold, et al, 2005 study, entitled: “The Circus Controversy”. “People have different views on animals performing in circuses. For example, some people think it is a great idea because it provides lots of entertainment for the public. Also, it gives parents and children something to do together, and the people who train the animals can make some money. However, other people think having animals in circuses is a bad idea because the animals are often locked in small cages and are not fed well. They also believe it is cruel to force a dog, tiger, or elephant to perform certain tricks that might be dangerous. I am interested in learning what you think about this controversy, and whether or not you think circuses with trained animals should be allowed to perform for the public. I would like you to spend the next 20 minutes writing an essay. Tell me exactly what you think about the controversy. Give me lots of good reasons for your opinion. Please use your best writing style, with correct grammar and spelling. If you aren’t sure how to spell a word, just take a guess.”(Nippold, Ward-Lonergan, & Fanning, 2005)
He produced the following written sample during the allotted 20 minutes.

Analysis: This student was able to generate a short, 3-paragraph, composition containing an introduction and a body without a definitive conclusion. His persuasive essay was judged to be very immature for his grade level due to significant disorganization, limited ability to support his point of view as well as the presence of tangential information in the introduction of his composition, which was significantly compromised by many writing mechanics errors (punctuation, capitalization, as well as spelling) that further impacted the coherence and cohesiveness of his written output.
The student’s introduction began with an inventive dialogue, which was irrelevant to the body of his persuasive essay. He did have three important points relevant to the body of the essay: animal cruelty, danger to the animals, and potential for the animals to harm humans. However, he was unable to adequately develop those points into full paragraphs. The notable absence of proofreading and editing of the composition further contributed to its lack of clarity. The above coupled with a lack of a conclusion was not commensurate grade-level expectations.
 Based on the above-written sample, the student’s persuasive composition content (thought formulation and elaboration) was judged to be significantly immature for his grade level and is commensurate with the abilities of a much younger student. The student’s composition contained several emerging claims that suggested a vague position. However, though the student attempted to back up his opinion and support his position (animals should not be performing in circuses), ultimately he was unable to do so in a coherent and cohesive manner.
Based on the above-written sample, the student’s persuasive composition content (thought formulation and elaboration) was judged to be significantly immature for his grade level and is commensurate with the abilities of a much younger student. The student’s composition contained several emerging claims that suggested a vague position. However, though the student attempted to back up his opinion and support his position (animals should not be performing in circuses), ultimately he was unable to do so in a coherent and cohesive manner.
Now that we know what the student’s written difficulties look like, the following goals will be applicable with respect to his writing remediation:
Long-Term Goals: Student will improve his written abilities for academic purposes.
- Short-Term Goals
- Student will appropriately utilize parts of speech (e.g., adjectives, adverbs, prepositions, etc.) in compound and complex sentences.
- Student will use a variety of sentence types for story composition purposes (e.g., declarative, interrogative, imperative, and exclamatory sentences).
- Student will correctly use past, present, and future verb tenses during writing tasks.
- Student will utilize appropriate punctuation at the sentence level (e.g., apostrophes, periods, commas, colons, quotation marks in dialogue, and apostrophes in singular possessives, etc.).
- Student will utilize appropriate capitalization at the sentence level (e.g., capitalize proper nouns, holidays, product names, titles with names, initials, geographic locations, historical periods, special events, etc.).
- Student will use prewriting techniques to generate writing ideas (e.g., list keywords, state key ideas, etc.).
- Student will determine the purpose of his writing and his intended audience in order to establish the tone of his writing as well as outline the main idea of his writing.
- Student will generate a draft in which information is organized in chronological order via use of temporal markers (e.g., “meanwhile,” “immediately”) as well as cohesive ties (e.g., ‘but’, ‘yet’, ‘so’, ‘nor’) and cause/effect transitions (e.g., “therefore,” “as a result”).
- Student will improve coherence and logical organization of his written output via the use of revision strategies (e.g., modify supporting details, use sentence variety, employ literary devices).
- Student will edit his draft for appropriate grammar, spelling, punctuation, and capitalization.
There you have it. A quick and easy qualitative writing assessment which can assist SLPs to determine the extent of the student’s writing difficulties as well as establish writing remediation targets for intervention purposes.
Using a different type of writing assessment with your students? Please share the details below so we can all benefit from each others knowledge of assessment strategies.
References:
- Nippold, M., Ward-Lonergan, J., & Fanning, J. (2005). Persuasive writing in children, adolescents, and adults: a study of syntactic, semantic, and pragmatic development. Language, Speech, and Hearing Services in Schools, 36, 125-138.
 Given the rising interest in recent years in the role of SLPs in the treatment of reading disorders, today I wanted to share with parents and professionals several reputable FREE resources on the subject of “dyslexia” in Russian-speaking children.
Given the rising interest in recent years in the role of SLPs in the treatment of reading disorders, today I wanted to share with parents and professionals several reputable FREE resources on the subject of “dyslexia” in Russian-speaking children. First up is the Report on the
First up is the Report on the  Next up is this delightful presentation entitled: “
Next up is this delightful presentation entitled: “ Now let us move on to the “
Now let us move on to the “

 For that purpose, Len is a good candidate for the administration of the
For that purpose, Len is a good candidate for the administration of the  Given Len’s reported history of narrative production deficits, Len is also a good candidate for the administration of the
Given Len’s reported history of narrative production deficits, Len is also a good candidate for the administration of the 
 Two years ago I wrote a blog post entitled: “
Two years ago I wrote a blog post entitled: “
 First up is the concept of learning vs. generalization. Here Dr. Kamhi discusses that some clinicians still possess an “outdated behavioral view of learning” in our field, which is not theoretically and clinically useful. He explains that when we are talking about generalization – what children truly have a difficulty with is “transferring narrow limited rules to new situations“. “Children with language and learning problems will have difficulty acquiring broad-based rules and modifying these rules once acquired, and they also will be more vulnerable to performance demands on speech production and comprehension (Kamhi, 1988)” (93). After all, it is not “reasonable to expect children to use language targets consistently after a brief period of intervention” and while we hope that “language intervention [is] designed to lead children with language disorders to acquire broad-based language rules” it is a hugely difficult task to undertake and execute.
First up is the concept of learning vs. generalization. Here Dr. Kamhi discusses that some clinicians still possess an “outdated behavioral view of learning” in our field, which is not theoretically and clinically useful. He explains that when we are talking about generalization – what children truly have a difficulty with is “transferring narrow limited rules to new situations“. “Children with language and learning problems will have difficulty acquiring broad-based rules and modifying these rules once acquired, and they also will be more vulnerable to performance demands on speech production and comprehension (Kamhi, 1988)” (93). After all, it is not “reasonable to expect children to use language targets consistently after a brief period of intervention” and while we hope that “language intervention [is] designed to lead children with language disorders to acquire broad-based language rules” it is a hugely difficult task to undertake and execute.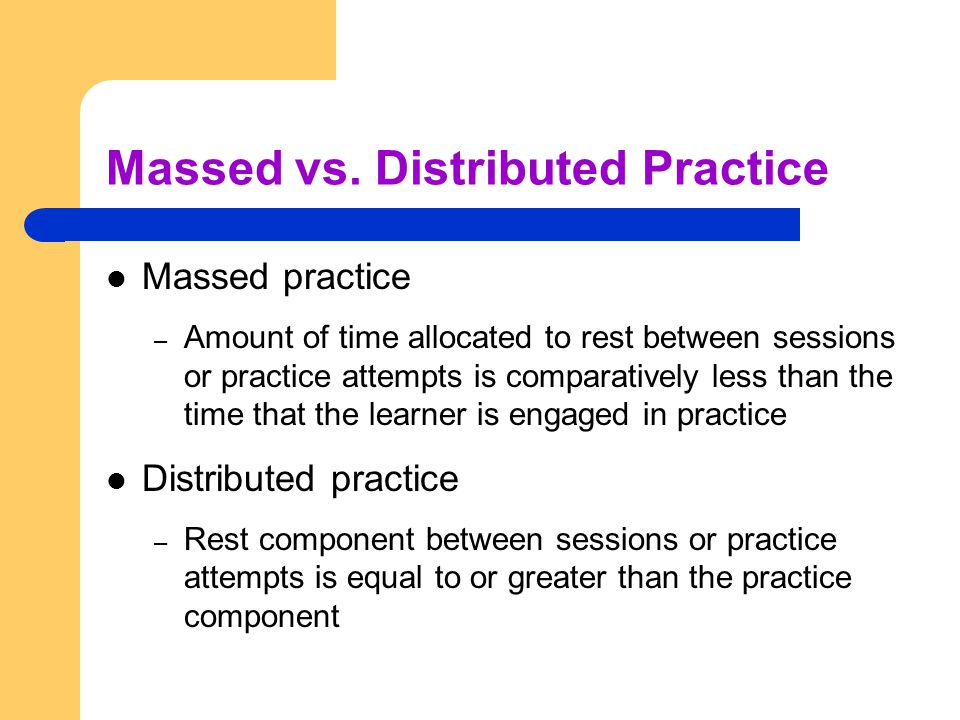 After that, Dr. Kamhi addresses the concept of distributed practice (spacing of intervention) and how important it is for teaching children with language disorders. He points out that a number of recent studies have found that “spacing and distribution of teaching episodes have more of an impact on treatment outcomes than
After that, Dr. Kamhi addresses the concept of distributed practice (spacing of intervention) and how important it is for teaching children with language disorders. He points out that a number of recent studies have found that “spacing and distribution of teaching episodes have more of an impact on treatment outcomes than 
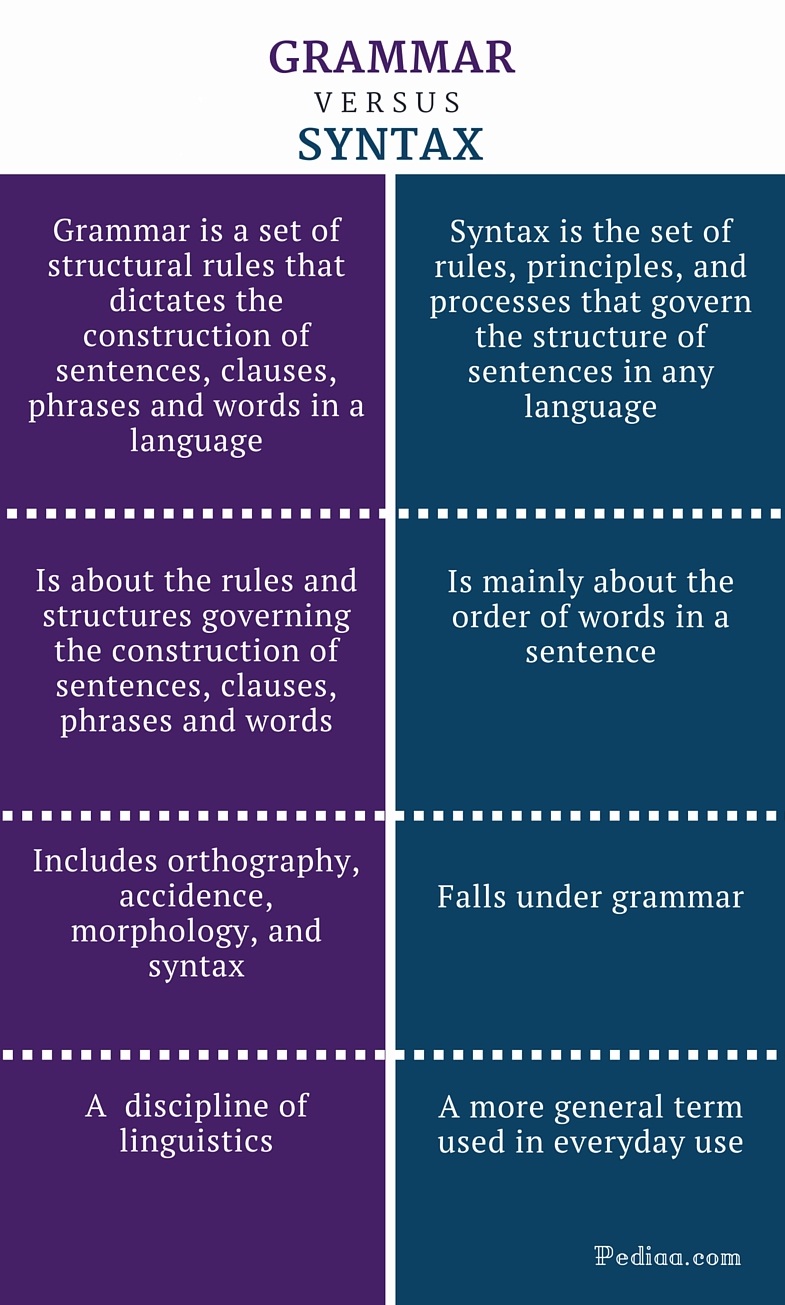 From there lets us take a look at Dr. Kamhi’s recommendations for grammar and syntax. Grammatical development goes much further than addressing Brown’s morphemes in therapy and calling it a day. As such, it is important to understand that children with developmental language disorders (DLD) (#DevLang) do not have difficulty acquiring all morphemes. Rather studies have shown that they have difficulty learning grammatical morphemes that reflect tense and agreement (e.g., third-person singular, past tense, auxiliaries, copulas, etc.). As such, use of measures developed by
From there lets us take a look at Dr. Kamhi’s recommendations for grammar and syntax. Grammatical development goes much further than addressing Brown’s morphemes in therapy and calling it a day. As such, it is important to understand that children with developmental language disorders (DLD) (#DevLang) do not have difficulty acquiring all morphemes. Rather studies have shown that they have difficulty learning grammatical morphemes that reflect tense and agreement (e.g., third-person singular, past tense, auxiliaries, copulas, etc.). As such, use of measures developed by  Dr. Kamhi supports the above point by providing an example of two passages. One, which describes a random order of events, and another which follows a logical order of events. He then points out that the randomly ordered story relies exclusively on attention and memory in terms of “sequencing”, while the second story reduces demands on memory due to its logical flow of events. As such, he points out that retelling deficits seemingly related to sequencing, tend to be actually due to “limitations in attention, working memory, and/or conceptual knowledge“. Hence, instead of targeting sequencing abilities in therapy, SLPs should instead use contextualized language intervention to target aspects of narrative development (macro and microstructural elements).
Dr. Kamhi supports the above point by providing an example of two passages. One, which describes a random order of events, and another which follows a logical order of events. He then points out that the randomly ordered story relies exclusively on attention and memory in terms of “sequencing”, while the second story reduces demands on memory due to its logical flow of events. As such, he points out that retelling deficits seemingly related to sequencing, tend to be actually due to “limitations in attention, working memory, and/or conceptual knowledge“. Hence, instead of targeting sequencing abilities in therapy, SLPs should instead use contextualized language intervention to target aspects of narrative development (macro and microstructural elements). There you have it! Ten practical suggestions from Dr. Kamhi ready for immediate implementation! And for more information, I highly recommend reading the other articles in the same
There you have it! Ten practical suggestions from Dr. Kamhi ready for immediate implementation! And for more information, I highly recommend reading the other articles in the same  I’ve always loved fairy tales! Much like Audrey Hepburn “If I’m honest I have to tell you I still read fairy-tales and I like them best of all.” Not to compare myself with Einstein (sadly in any way, sigh) but “When I examine myself and my methods of thought, I come to the conclusion that the gift of fantasy has meant more to me than any talent for abstract, positive thinking.”
I’ve always loved fairy tales! Much like Audrey Hepburn “If I’m honest I have to tell you I still read fairy-tales and I like them best of all.” Not to compare myself with Einstein (sadly in any way, sigh) but “When I examine myself and my methods of thought, I come to the conclusion that the gift of fantasy has meant more to me than any talent for abstract, positive thinking.” Those of us who have administered PLS-5 ever since its release in 2011, know that the test is fraught with significant psychometric problems. Previous reviews of its poor sensitivity, specificity, validity, and reliability, have been extensively discussed
Those of us who have administered PLS-5 ever since its release in 2011, know that the test is fraught with significant psychometric problems. Previous reviews of its poor sensitivity, specificity, validity, and reliability, have been extensively discussed 

 Today I want to talk treatment. That thing that we need to plan for as we are doing our assessments. But are we starting our treatments the right way? The answer may surprise you. I often see SLPs phrasing questions regarding treatment the following way: “I have a student diagnosed with ____ (insert disorder here). What is everyone using (program/app/materials) during therapy sessions to address ___ diagnosis?”
Today I want to talk treatment. That thing that we need to plan for as we are doing our assessments. But are we starting our treatments the right way? The answer may surprise you. I often see SLPs phrasing questions regarding treatment the following way: “I have a student diagnosed with ____ (insert disorder here). What is everyone using (program/app/materials) during therapy sessions to address ___ diagnosis?” There could be endless variations of how deficits manifest in poor readers. Is it aspects of phonological awareness, phonics, morphology, etc. What combination of deficits is preventing the child from becoming a good reader?
There could be endless variations of how deficits manifest in poor readers. Is it aspects of phonological awareness, phonics, morphology, etc. What combination of deficits is preventing the child from becoming a good reader? Reading Fluency: “LG’s reading fluency during this task was judged to be significantly affected by excessive speed, inappropriate pausing, word misreadings, choppy prosody, as well as inefficient word attack skills. While she was able to limitedly utilize the phonetic spelling of unfamiliar words (e.g., __) provided to her in parenthesis next to the word (which she initially misread as ‘__’), she exhibited limited use of metalinguistic strategies (e.g., pre-scanning sentences to aid text comprehension, self-correcting to ensure that the read words made sense in the context of the sentence, etc.), when reading the provided passage. To illustrate, during the reading of the text, LG was observed to frequently (at least 3 times) lose her place and skip entire lines of text without any attempts at self-correction. At times she was observed to read the same word a number of different ways (e.g., read ‘soup’ as ‘soup’ then as ‘soap’, ‘roots’ as ‘roofs’ then as ‘roots’, etc.) without attempting to self-correct. LG’s oral reading rate was also observed to be impaired for her age/grade levels. Her prosody was significantly adversely affected due to lack of adequate pausing for punctuation marks (e.g., periods, commas, etc.). Instead, she paused during text reading only when he could not decode select words in the text. Though, LG was able to read 70 words per minute, which was judged to be grossly commensurate with grade-level, out of these 70 words she skipped 2 entire lines of text, invented an entire line of text, as well as made 4 decoding errors and 6 inappropriate pauses.”
Reading Fluency: “LG’s reading fluency during this task was judged to be significantly affected by excessive speed, inappropriate pausing, word misreadings, choppy prosody, as well as inefficient word attack skills. While she was able to limitedly utilize the phonetic spelling of unfamiliar words (e.g., __) provided to her in parenthesis next to the word (which she initially misread as ‘__’), she exhibited limited use of metalinguistic strategies (e.g., pre-scanning sentences to aid text comprehension, self-correcting to ensure that the read words made sense in the context of the sentence, etc.), when reading the provided passage. To illustrate, during the reading of the text, LG was observed to frequently (at least 3 times) lose her place and skip entire lines of text without any attempts at self-correction. At times she was observed to read the same word a number of different ways (e.g., read ‘soup’ as ‘soup’ then as ‘soap’, ‘roots’ as ‘roofs’ then as ‘roots’, etc.) without attempting to self-correct. LG’s oral reading rate was also observed to be impaired for her age/grade levels. Her prosody was significantly adversely affected due to lack of adequate pausing for punctuation marks (e.g., periods, commas, etc.). Instead, she paused during text reading only when he could not decode select words in the text. Though, LG was able to read 70 words per minute, which was judged to be grossly commensurate with grade-level, out of these 70 words she skipped 2 entire lines of text, invented an entire line of text, as well as made 4 decoding errors and 6 inappropriate pauses.”
