 Picture books are absolutely wonderful for both assessment and treatment purposes! They are terrific as narrative elicitation aids for children of various ages, ranging from pre-K through fourth grade. They are amazing treatment aids for addressing a variety of speech, language, and literacy goals that extend far beyond narrative production. Continue reading Speech, Language, and Literacy Fun with Helen Lester’s Picture Books
Picture books are absolutely wonderful for both assessment and treatment purposes! They are terrific as narrative elicitation aids for children of various ages, ranging from pre-K through fourth grade. They are amazing treatment aids for addressing a variety of speech, language, and literacy goals that extend far beyond narrative production. Continue reading Speech, Language, and Literacy Fun with Helen Lester’s Picture Books
Category: language delay
Tips on Reducing ‘Summer Learning Loss’ in Children with Language/Literacy Disorders
 The end of the school year is almost near. Soon many of our clients with language and literacy difficulties will be going on summer vacation and enjoying their time outside of school. However, summer is not all fun and games. For children with learning needs, this is also a time of “learning loss”, or the loss of academic skills and knowledge over the course of the summer break. Students diagnosed with language and learning disabilities are at a particularly significant risk of greater learning loss than typically developing students. Continue reading Tips on Reducing ‘Summer Learning Loss’ in Children with Language/Literacy Disorders
The end of the school year is almost near. Soon many of our clients with language and literacy difficulties will be going on summer vacation and enjoying their time outside of school. However, summer is not all fun and games. For children with learning needs, this is also a time of “learning loss”, or the loss of academic skills and knowledge over the course of the summer break. Students diagnosed with language and learning disabilities are at a particularly significant risk of greater learning loss than typically developing students. Continue reading Tips on Reducing ‘Summer Learning Loss’ in Children with Language/Literacy Disorders
Assessing Social Pragmatic Abilities in Children with Language Difficulties
You’ve received a referral to assess the language abilities of a school aged child with suspected language difficulties. The child has not been assessed before so you know you’ll need a comprehensive language test to look at the child’s ability to recall sentences, follow directions, name words, as well as perform a number of other tasks showcasing the child’s abilities in the areas of content and form (Bloom & Lahey, 1978).
But how about the area of language use? Will you be assessing the child’s pragmatic and social cognitive abilities as well during your language assessment? After all most comprehensive standardized assessments, “typically focus on semantics, syntax, morphology, and phonology, as these are the performance areas in which specific skill development can be most objectively measured” (Hill & Coufal, 2005, p 35). Continue reading Assessing Social Pragmatic Abilities in Children with Language Difficulties
On the Disadvantages of Parents Ceasing to Speak the Birth Language with Bilingual Language Impaired Children
 Despite significant advances in the fields of education and speech pathology, many harmful myths pertaining to multilingualism continue to persist. One particularly infuriating and patently incorrect recommendation to parents is the advice to stop speaking the birth language with their bilingual children with language disorders. Continue reading On the Disadvantages of Parents Ceasing to Speak the Birth Language with Bilingual Language Impaired Children
Despite significant advances in the fields of education and speech pathology, many harmful myths pertaining to multilingualism continue to persist. One particularly infuriating and patently incorrect recommendation to parents is the advice to stop speaking the birth language with their bilingual children with language disorders. Continue reading On the Disadvantages of Parents Ceasing to Speak the Birth Language with Bilingual Language Impaired Children
FREE Resources for Working with Russian Speaking Clients: Part II
A few years ago I wrote a blog post entitled “Working with Russian-speaking clients: implications for speech-language assessment” the aim of which was to provide some suggestions regarding assessment of bilingual Russian-American birth-school age population in order to assist SLPs with determining whether the assessed child presents with a language difference, insufficient language exposure, or a true language disorder.
Today I wanted to provide Russian speaking clinicians with a few FREE resources pertaining to the typical speech and language development of Russian speaking children 0-7 years of age.
Below materials include several FREE questionnaires regarding Russian language development (words and sentences) of children 0-3 years of age, a parent intake forms for Russian speaking clients, as well as a few relevant charts pertaining to the development of phonology, word formation, lexicon, morphology, syntax, and metalinguistics of children 0-7 years of age.
It is, however, important to note that due to the absence of research and standardized studies on this subject much of the below information still needs to be interpreted with significant caution.
Select Speech and Language Norms:
- Некоторые нормативы речевого развития детей от 18 до 36 месяцев (по материалам МакАртуровского опросника) (Number of words and sentence per age of Russian speakign children based on McArthur Bates)
- Речевой онтогенез: Развитие Речи Ребенка В Норме 0-7 years of age (based on the work of А.Н. Гвоздев) includes: Фонетика,Словообразование, Лексика, Морфолог-ия, Синтаксис, Метаязыковая деятельность (phonology, word formation, lexicon, morphology, syntax, and metalinguistics)
- Развитиe связной речи у детей 3-7 лет
a. Составление рассказа по серии сюжетных картинок
b. Пересказ текста
c. Составление описательного рассказа

Select Parent Questionnaires (McArthur Bates Adapted in Russian):
- Тест речевого и коммуникативного развития детей раннего возраста: слова и жесты (Words and Gestures)
- Тест речевого и коммуникативного развития детей раннего возраста: слова и предложения (Sentences)
- Анкета для родителей (Child Development Questionnaire for Parents)
Материал Для Родителей И Специалистов По Речевым
Нарушениям contains detailed information (27 pages) on Russian child development as well as common communication disrupting disorders
Stay tuned for more resources for Russian speaking SLPs coming shortly.
Related Resources:
- Working with Russian-speaking clients: implications for speech-language assessment
- Assessment of sound and syllable imitation in Russian speaking infants and toddlers
- Russian Articulation Screener
- Language Difference vs. Language Disorder: Assessment & Intervention Strategies for SLPs Working with Bilingual Children
- Impact of Cultural and Linguistic Variables On Speech-Language Services
It’s All Due to …Language: How Subtle Symptoms Can Cause Serious Academic Deficits
 Scenario: Len is a 7-2-year-old, 2nd-grade student who struggles with reading and writing in the classroom. He is very bright and has a high average IQ, yet when he is speaking he frequently can’t get his point across to others due to excessive linguistic reformulations and word-finding difficulties. The problem is that Len passed all the typical educational and language testing with flying colors, receiving average scores across the board on various tests including the Woodcock-Johnson Fourth Edition (WJ-IV) and the Clinical Evaluation of Language Fundamentals-5 (CELF-5). Stranger still is the fact that he aced Comprehensive Test of Phonological Processing, Second Edition (CTOPP-2), with flying colors, so he is not even eligible for a “dyslexia” diagnosis. Len is clearly struggling in the classroom with coherently expressing self, telling stories, understanding what he is reading, as well as putting his thoughts on paper. His parents have compiled impressively huge folders containing examples of his struggles. Yet because of his performance on the basic standardized assessment batteries, Len does not qualify for any functional assistance in the school setting, despite being virtually functionally illiterate in second grade.
Scenario: Len is a 7-2-year-old, 2nd-grade student who struggles with reading and writing in the classroom. He is very bright and has a high average IQ, yet when he is speaking he frequently can’t get his point across to others due to excessive linguistic reformulations and word-finding difficulties. The problem is that Len passed all the typical educational and language testing with flying colors, receiving average scores across the board on various tests including the Woodcock-Johnson Fourth Edition (WJ-IV) and the Clinical Evaluation of Language Fundamentals-5 (CELF-5). Stranger still is the fact that he aced Comprehensive Test of Phonological Processing, Second Edition (CTOPP-2), with flying colors, so he is not even eligible for a “dyslexia” diagnosis. Len is clearly struggling in the classroom with coherently expressing self, telling stories, understanding what he is reading, as well as putting his thoughts on paper. His parents have compiled impressively huge folders containing examples of his struggles. Yet because of his performance on the basic standardized assessment batteries, Len does not qualify for any functional assistance in the school setting, despite being virtually functionally illiterate in second grade.
The truth is that Len is quite a familiar figure to many SLPs, who at one time or another have encountered such a student and asked for guidance regarding the appropriate accommodations and services for him on various SLP-geared social media forums. But what makes Len such an enigma, one may inquire? Surely if the child had tangible deficits, wouldn’t standardized testing at least partially reveal them?
Well, it all depends really, on what type of testing was administered to Len in the first place. A few years ago I wrote a post entitled: “What Research Shows About the Functional Relevance of Standardized Language Tests“. What researchers found is that there is a “lack of a correlation between frequency of test use and test accuracy, measured both in terms of sensitivity/specificity and mean difference scores” (Betz et al, 2012, 141). Furthermore, they also found that the most frequently used tests were the comprehensive assessments including the Clinical Evaluation of Language Fundamentals and the Preschool Language Scale as well as one-word vocabulary tests such as the Peabody Picture Vocabulary Test”. Most damaging finding was the fact that: “frequently SLPs did not follow up the comprehensive standardized testing with domain-specific assessments (critical thinking, social communication, etc.) but instead used the vocabulary testing as a second measure”.(Betz et al, 2012, 140)
In other words, many SLPs only use the tests at hand rather than the RIGHT tests aimed at identifying the student’s specific deficits. But the problem doesn’t actually stop there. Due to the variation in psychometric properties of various tests, many children with language impairment are overlooked by standardized tests by receiving scores within the average range or not receiving low enough scores to qualify for services.
Thus, “the clinical consequence is that a child who truly has a language impairment has a roughly equal chance of being correctly or incorrectly identified, depending on the test that he or she is given.” Furthermore, “even if a child is diagnosed accurately as language impaired at one point in time, future diagnoses may lead to the false perception that the child has recovered, depending on the test(s) that he or she has been given (Spaulding, Plante & Farinella, 2006, 69).”
There’s of course yet another factor affecting our hypothetical client and that is his relatively young age. This is especially evident with many educational and language testing for children in the 5-7 age group. Because the bar is set so low, concept-wise for these age-groups, many children with moderate language and literacy deficits can pass these tests with flying colors, only to be flagged by them literally two years later and be identified with deficits, far too late in the game. Coupled with the fact that many SLPs do not utilize non-standardized measures to supplement their assessments, Len is in a pretty serious predicament.
But what if there was a do-over? What could we do differently for Len to rectify this situation? For starters, we need to pay careful attention to his deficits profile in order to choose appropriate tests to evaluate his areas of needs. The above can be accomplished via a number of ways. The SLP can interview Len’s teacher and his caregiver/s in order to obtain a summary of his pressing deficits. Depending on the extent of the reported deficits the SLP can also provide them with a referral checklist to mark off the most significant areas of need.
In Len’s case, we already have a pretty good idea regarding what’s going on. We know that he passed basic language and educational testing, so in the words of Dr. Geraldine Wallach, we need to keep “peeling the onion” via the administration of more sensitive tests to tap into Len’s reported areas of deficits which include: word-retrieval, narrative production, as well as reading and writing.
 For that purpose, Len is a good candidate for the administration of the Test of Integrated Language and Literacy (TILLS), which was developed to identify language and literacy disorders, has good psychometric properties, and contains subtests for assessment of relevant skills such as reading fluency, reading comprehension, phonological awareness, spelling, as well as writing in school-age children.
For that purpose, Len is a good candidate for the administration of the Test of Integrated Language and Literacy (TILLS), which was developed to identify language and literacy disorders, has good psychometric properties, and contains subtests for assessment of relevant skills such as reading fluency, reading comprehension, phonological awareness, spelling, as well as writing in school-age children.
 Given Len’s reported history of narrative production deficits, Len is also a good candidate for the administration of the Social Language Development Test Elementary (SLDTE). Here’s why. Research indicates that narrative weaknesses significantly correlate with social communication deficits (Norbury, Gemmell & Paul, 2014). As such, it’s not just children with Autism Spectrum Disorders who present with impaired narrative abilities. Many children with developmental language impairment (DLD) (#devlangdis) can present with significant narrative deficits affecting their social and academic functioning, which means that their social communication abilities need to be tested to confirm/rule out presence of these difficulties.
Given Len’s reported history of narrative production deficits, Len is also a good candidate for the administration of the Social Language Development Test Elementary (SLDTE). Here’s why. Research indicates that narrative weaknesses significantly correlate with social communication deficits (Norbury, Gemmell & Paul, 2014). As such, it’s not just children with Autism Spectrum Disorders who present with impaired narrative abilities. Many children with developmental language impairment (DLD) (#devlangdis) can present with significant narrative deficits affecting their social and academic functioning, which means that their social communication abilities need to be tested to confirm/rule out presence of these difficulties.
However, standardized tests are not enough, since even the best-standardized tests have significant limitations. As such, several non-standardized assessments in the areas of narrative production, reading, and writing, may be recommended for Len to meaningfully supplement his testing.
Let’s begin with an informal narrative assessment which provides detailed information regarding microstructural and macrostructural aspects of storytelling as well as child’s thought processes and socio-emotional functioning. My nonstandardized narrative assessments are based on the book elicitation recommendations from the SALT website. For 2nd graders, I use the book by Helen Lester entitled Pookins Gets Her Way. I first read the story to the child, then cover up the words and ask the child to retell the story based on pictures. I read the story first because: “the model narrative presents the events, plot structure, and words that the narrator is to retell, which allows more reliable scoring than a generated story that can go in many directions” (Allen et al, 2012, p. 207).
As the child is retelling his story I digitally record him using the Voice Memos application on my iPhone, for a later transcription and thorough analysis. During storytelling, I only use the prompts: ‘What else can you tell me?’ and ‘Can you tell me more?’ to elicit additional information. I try not to prompt the child excessively since I am interested in cataloging all of his narrative-based deficits. After I transcribe the sample, I analyze it and make sure that I include the transcription and a detailed write-up in the body of my report, so parents and professionals can see and understand the nature of the child’s errors/weaknesses.
 Now we are ready to move on to a brief nonstandardized reading assessment. For this purpose, I often use the books from the Continental Press series entitled: Reading for Comprehension, which contains books for grades 1-8. After I confirm with either the parent or the child’s teacher that the selected passage is reflective of the complexity of work presented in the classroom for his grade level, I ask the child to read the text. As the child is reading, I calculate the correct number of words he reads per minute as well as what type of errors the child is exhibiting during reading. Then I ask the child to state the main idea of the text, summarize its key points as well as define select text embedded vocabulary words and answer a few, verbally presented reading comprehension questions. After that, I provide the child with accompanying 5 multiple choice question worksheet and ask the child to complete it. I analyze my results in order to determine whether I have accurately captured the child’s reading profile.
Now we are ready to move on to a brief nonstandardized reading assessment. For this purpose, I often use the books from the Continental Press series entitled: Reading for Comprehension, which contains books for grades 1-8. After I confirm with either the parent or the child’s teacher that the selected passage is reflective of the complexity of work presented in the classroom for his grade level, I ask the child to read the text. As the child is reading, I calculate the correct number of words he reads per minute as well as what type of errors the child is exhibiting during reading. Then I ask the child to state the main idea of the text, summarize its key points as well as define select text embedded vocabulary words and answer a few, verbally presented reading comprehension questions. After that, I provide the child with accompanying 5 multiple choice question worksheet and ask the child to complete it. I analyze my results in order to determine whether I have accurately captured the child’s reading profile.
Finally, if any additional information is needed, I administer a nonstandardized writing assessment, which I base on the Common Core State Standards for 2nd grade. For this task, I provide a student with a writing prompt common for second grade and give him a period of 15-20 minutes to generate a writing sample. I then analyze the writing sample with respect to contextual conventions (punctuation, capitalization, grammar, and syntax) as well as story composition (overall coherence and cohesion of the written sample).
The above relatively short assessment battery (2 standardized tests and 3 informal assessment tasks) which takes approximately 2-2.5 hours to administer, allows me to create a comprehensive profile of the child’s language and literacy strengths and needs. It also allows me to generate targeted goals in order to begin effective and meaningful remediation of the child’s deficits.
Children like Len will, unfortunately, remain unidentified unless they are administered more sensitive tasks to better understand their subtle pattern of deficits. Consequently, to ensure that they do not fall through the cracks of our educational system due to misguided overreliance on a limited number of standardized assessments, it is very important that professionals select the right assessments, rather than the assessments at hand, in order to accurately determine the child’s areas of needs.
References:
- Allen, M, Ukrainetz, T & Carswell, A (2012) The narrative language performance of three types of at-risk first-grade readers. Language, Speech, and Hearing Services in Schools, 43(2), 205-221.
- Betz et al. (2013) Factors Influencing the Selection of Standardized Tests for the Diagnosis of Specific Language Impairment. Language, Speech, and Hearing Services in Schools, 44, 133-146.
- Hasbrouck, J. & Tindal, G. A. (2006). Oral reading fluency norms: A valuable assessment tool for reading teachers. The Reading Teacher. 59(7), 636-644.).
- Norbury, C. F., Gemmell, T., & Paul, R. (2014). Pragmatics abilities in narrative production: a cross-disorder comparison. Journal of child language, 41(03), 485-510.
- Peña, E.D., Spaulding, T.J., & Plante, E. (2006). The Composition of Normative Groups and Diagnostic Decision Making: Shooting Ourselves in the Foot. American Journal of Speech-Language Pathology, 15, 247-254.
- Spaulding, Plante & Farinella (2006) Eligibility Criteria for Language Impairment: Is the Low End of Normal Always Appropriate? Language, Speech, and Hearing Services in Schools, 37, 61-72.
- Spaulding, Szulga, & Figueria (2012) Using Norm-Referenced Tests to Determine Severity of Language Impairment in Children: Disconnect Between U.S. Policy Makers and Test Developers. Journal of Speech, Language and Hearing Research. 43, 176-190.
Making Our Interventions Count or What’s Research Got To Do With It?
 Two years ago I wrote a blog post entitled: “What’s Memes Got To Do With It?” which summarized key points of Dr. Alan G. Kamhi’s 2004 article: “A Meme’s Eye View of Speech-Language Pathology“. It delved into answering the following question: “Why do some terms, labels, ideas, and constructs [in our field] prevail whereas others fail to gain acceptance?”.
Two years ago I wrote a blog post entitled: “What’s Memes Got To Do With It?” which summarized key points of Dr. Alan G. Kamhi’s 2004 article: “A Meme’s Eye View of Speech-Language Pathology“. It delved into answering the following question: “Why do some terms, labels, ideas, and constructs [in our field] prevail whereas others fail to gain acceptance?”.
Today I would like to reference another article by Dr. Kamhi written in 2014, entitled “Improving Clinical Practices for Children With Language and Learning Disorders“.
This article was written to address the gaps between research and clinical practice with respect to the implementation of EBP for intervention purposes.
Dr. Kamhi begins the article by posing 10 True or False questions for his readers:
- Learning is easier than generalization.
- Instruction that is constant and predictable is more effective than instruction that varies the conditions of learning and practice.
- Focused stimulation (massed practice) is a more effective teaching strategy than varied stimulation (distributed practice).
- The more feedback, the better.
- Repeated reading of passages is the best way to learn text information.
- More therapy is always better.
- The most effective language and literacy interventions target processing limitations rather than knowledge deficits.
- Telegraphic utterances (e.g., push ball, mommy sock) should not be provided as input for children with limited language.
- Appropriate language goals include increasing levels of mean length of utterance (MLU) and targeting Brown’s (1973) 14 grammatical morphemes.
- Sequencing is an important skill for narrative competence.
Guess what? Only statement 8 of the above quiz is True! Every other statement from the above is FALSE!
Now, let’s talk about why that is!
 First up is the concept of learning vs. generalization. Here Dr. Kamhi discusses that some clinicians still possess an “outdated behavioral view of learning” in our field, which is not theoretically and clinically useful. He explains that when we are talking about generalization – what children truly have a difficulty with is “transferring narrow limited rules to new situations“. “Children with language and learning problems will have difficulty acquiring broad-based rules and modifying these rules once acquired, and they also will be more vulnerable to performance demands on speech production and comprehension (Kamhi, 1988)” (93). After all, it is not “reasonable to expect children to use language targets consistently after a brief period of intervention” and while we hope that “language intervention [is] designed to lead children with language disorders to acquire broad-based language rules” it is a hugely difficult task to undertake and execute.
First up is the concept of learning vs. generalization. Here Dr. Kamhi discusses that some clinicians still possess an “outdated behavioral view of learning” in our field, which is not theoretically and clinically useful. He explains that when we are talking about generalization – what children truly have a difficulty with is “transferring narrow limited rules to new situations“. “Children with language and learning problems will have difficulty acquiring broad-based rules and modifying these rules once acquired, and they also will be more vulnerable to performance demands on speech production and comprehension (Kamhi, 1988)” (93). After all, it is not “reasonable to expect children to use language targets consistently after a brief period of intervention” and while we hope that “language intervention [is] designed to lead children with language disorders to acquire broad-based language rules” it is a hugely difficult task to undertake and execute.
Next, Dr. Kamhi addresses the issue of instructional factors, specifically the importance of “varying conditions of instruction and practice“. Here, he addresses the fact that while contextualized instruction is highly beneficial to learners unless we inject variability and modify various aspects of instruction including context, composition, duration, etc., we ran the risk of limiting our students’ long-term outcomes.
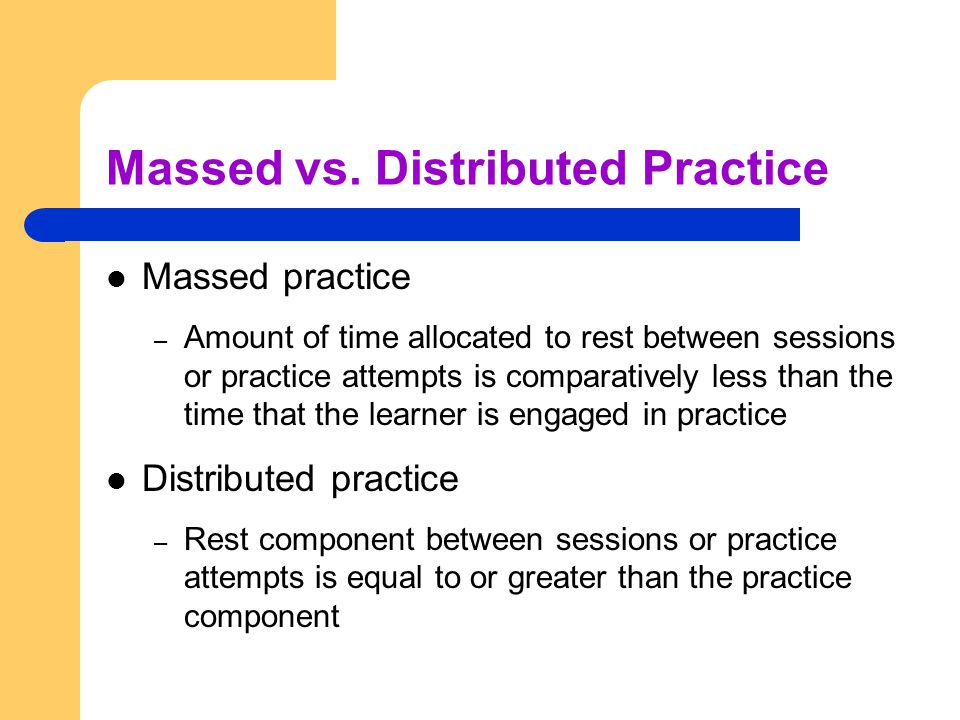 After that, Dr. Kamhi addresses the concept of distributed practice (spacing of intervention) and how important it is for teaching children with language disorders. He points out that a number of recent studies have found that “spacing and distribution of teaching episodes have more of an impact on treatment outcomes than treatment intensity” (94).
After that, Dr. Kamhi addresses the concept of distributed practice (spacing of intervention) and how important it is for teaching children with language disorders. He points out that a number of recent studies have found that “spacing and distribution of teaching episodes have more of an impact on treatment outcomes than treatment intensity” (94).
He also advocates reducing evaluative feedback to learners to “enhance long-term retention and generalization of motor skills“. While he cites research from studies pertaining to speech production, he adds that language learning could also benefit from this practice as it would reduce conversational disruptions and tunning out on the part of the student.
From there he addresses the limitations of repetition for specific tasks (e.g., text rereading). He emphasizes how important it is for students to recall and retrieve text rather than repeatedly reread it (even without correction), as the latter results in a lack of comprehension/retention of read information.
After that, he discusses treatment intensity. Here he emphasizes the fact that higher dose of instruction will not necessarily result in better therapy outcomes due to the research on the effects of “learning plateaus and threshold effects in language and literacy” (95). We have seen research on this with respect to joint book reading, vocabulary words exposure, etc. As such, at a certain point in time increased intensity may actually result in decreased treatment benefits.
 His next point against processing interventions is very near and dear to my heart. Those of you familiar with my blog know that I have devoted a substantial number of posts pertaining to the lack of validity of CAPD diagnosis (as a standalone entity) and urged clinicians to provide language based vs. specific auditory interventions which lack treatment utility. Here, Dr. Kamhi makes a great point that: “Interventions that target processing skills are particularly appealing because they offer the promise of improving language and learning deficits without having to directly target the specific knowledge and skills required to be a proficient speaker, listener, reader, and writer.” (95) The problem is that we have numerous studies on the topic of improvement of isolated skills (e.g., auditory skills, working memory, slow processing, etc.) which clearly indicate lack of effectiveness of these interventions. As such, “practitioners should be highly skeptical of interventions that promise quick fixes for language and learning disabilities” (96).
His next point against processing interventions is very near and dear to my heart. Those of you familiar with my blog know that I have devoted a substantial number of posts pertaining to the lack of validity of CAPD diagnosis (as a standalone entity) and urged clinicians to provide language based vs. specific auditory interventions which lack treatment utility. Here, Dr. Kamhi makes a great point that: “Interventions that target processing skills are particularly appealing because they offer the promise of improving language and learning deficits without having to directly target the specific knowledge and skills required to be a proficient speaker, listener, reader, and writer.” (95) The problem is that we have numerous studies on the topic of improvement of isolated skills (e.g., auditory skills, working memory, slow processing, etc.) which clearly indicate lack of effectiveness of these interventions. As such, “practitioners should be highly skeptical of interventions that promise quick fixes for language and learning disabilities” (96).
Now let us move on to language and particularly the models we provide to our clients to encourage greater verbal output. Research indicates that when clinicians are attempting to expand children’s utterances, they need to provide well-formed language models. Studies show that children select strong input when its surrounded by weaker input (the surrounding weaker syllables make stronger syllables stand out). As such, clinicians should expand upon/comment on what clients are saying with grammatically complete models vs. telegraphic productions.
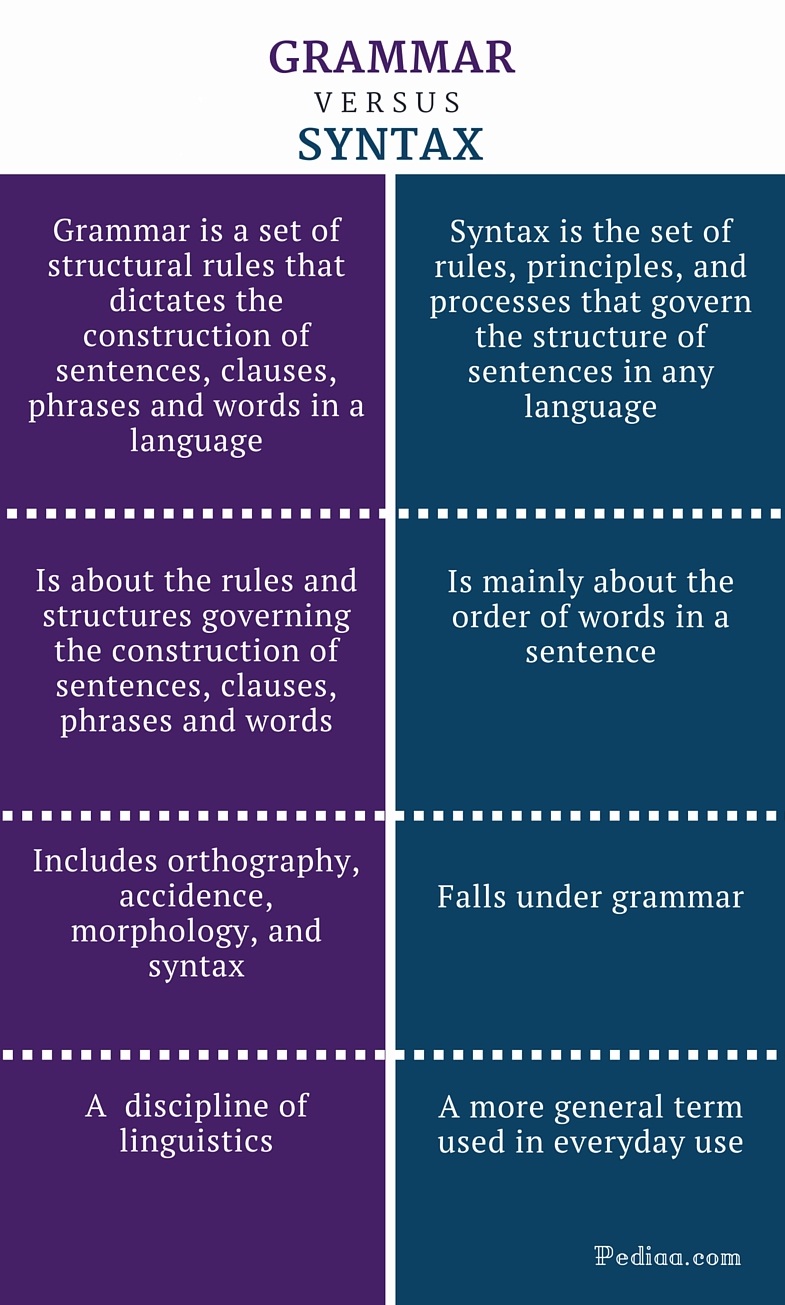 From there lets us take a look at Dr. Kamhi’s recommendations for grammar and syntax. Grammatical development goes much further than addressing Brown’s morphemes in therapy and calling it a day. As such, it is important to understand that children with developmental language disorders (DLD) (#DevLang) do not have difficulty acquiring all morphemes. Rather studies have shown that they have difficulty learning grammatical morphemes that reflect tense and agreement (e.g., third-person singular, past tense, auxiliaries, copulas, etc.). As such, use of measures developed by Hadley & Holt, 2006; Hadley & Short, 2005 (e.g., Tense Marker Total & Productivity Score) can yield helpful information regarding which grammatical structures to target in therapy.
From there lets us take a look at Dr. Kamhi’s recommendations for grammar and syntax. Grammatical development goes much further than addressing Brown’s morphemes in therapy and calling it a day. As such, it is important to understand that children with developmental language disorders (DLD) (#DevLang) do not have difficulty acquiring all morphemes. Rather studies have shown that they have difficulty learning grammatical morphemes that reflect tense and agreement (e.g., third-person singular, past tense, auxiliaries, copulas, etc.). As such, use of measures developed by Hadley & Holt, 2006; Hadley & Short, 2005 (e.g., Tense Marker Total & Productivity Score) can yield helpful information regarding which grammatical structures to target in therapy.
With respect to syntax, Dr. Kamhi notes that many clinicians erroneously believe that complex syntax should be targeted when children are much older. The Common Core State Standards do not help this cause further, since according to the CCSS complex syntax should be targeted 2-3 grades, which is far too late. Typically developing children begin developing complex syntax around 2 years of age and begin readily producing it around 3 years of age. As such, clinicians should begin targeting complex syntax in preschool years and not wait until the children have mastered all morphemes and clauses (97)
Finally, Dr. Kamhi wraps up his article by offering suggestions regarding prioritizing intervention goals. Here, he explains that goal prioritization is affected by
- clinician experience and competencies
- the degree of collaboration with other professionals
- type of service delivery model
- client/student factors
He provides a hypothetical case scenario in which the teaching responsibilities are divvied up between three professionals, with SLP in charge of targeting narrative discourse. Here, he explains that targeting narratives does not involve targeting sequencing abilities. “The ability to understand and recall events in a story or script depends on conceptual understanding of the topic and attentional/memory abilities, not sequencing ability.” He emphasizes that sequencing is not a distinct cognitive process that requires isolated treatment. Yet many SLPs “continue to believe that sequencing is a distinct processing skill that needs to be assessed and treated.” (99)
 Dr. Kamhi supports the above point by providing an example of two passages. One, which describes a random order of events, and another which follows a logical order of events. He then points out that the randomly ordered story relies exclusively on attention and memory in terms of “sequencing”, while the second story reduces demands on memory due to its logical flow of events. As such, he points out that retelling deficits seemingly related to sequencing, tend to be actually due to “limitations in attention, working memory, and/or conceptual knowledge“. Hence, instead of targeting sequencing abilities in therapy, SLPs should instead use contextualized language intervention to target aspects of narrative development (macro and microstructural elements).
Dr. Kamhi supports the above point by providing an example of two passages. One, which describes a random order of events, and another which follows a logical order of events. He then points out that the randomly ordered story relies exclusively on attention and memory in terms of “sequencing”, while the second story reduces demands on memory due to its logical flow of events. As such, he points out that retelling deficits seemingly related to sequencing, tend to be actually due to “limitations in attention, working memory, and/or conceptual knowledge“. Hence, instead of targeting sequencing abilities in therapy, SLPs should instead use contextualized language intervention to target aspects of narrative development (macro and microstructural elements).
Furthermore, here it is also important to note that the “sequencing fallacy” affects more than just narratives. It is very prevalent in the intervention process in the form of the ubiquitous “following directions” goal/s. Many clinicians readily create this goal for their clients due to their belief that it will result in functional therapeutic language gains. However, when one really begins to deconstruct this goal, one will realize that it involves a number of discrete abilities including: memory, attention, concept knowledge, inferencing, etc. Consequently, targeting the above goal will not result in any functional gains for the students (their memory abilities will not magically improve as a result of it). Instead, targeting specific language and conceptual goals (e.g., answering questions, producing complex sentences, etc.) and increasing the students’ overall listening comprehension and verbal expression will result in improvements in the areas of attention, memory, and processing, including their ability to follow complex directions.
 There you have it! Ten practical suggestions from Dr. Kamhi ready for immediate implementation! And for more information, I highly recommend reading the other articles in the same clinical forum, all of which possess highly practical and relevant ideas for therapeutic implementation. They include:
There you have it! Ten practical suggestions from Dr. Kamhi ready for immediate implementation! And for more information, I highly recommend reading the other articles in the same clinical forum, all of which possess highly practical and relevant ideas for therapeutic implementation. They include:
- Clinical Scientists Improving Clinical Practices: In Thoughts and Actions
- Approaching Early Grammatical Intervention From a Sentence-Focused Framework
- What Works in Therapy: Further Thoughts on Improving Clinical Practice for Children With Language Disorders
- Improving Clinical Practice: A School-Age and School-Based Perspective
- Improving Clinical Services: Be Aware of Fuzzy Connections Between Principles and Strategies
- One Size Does Not Fit All: Improving Clinical Practice in Older Children and Adolescents With Language and Learning Disorders
- Language Intervention at the Middle School: Complex Talk Reflects Complex Thought
- Using Our Knowledge of Typical Language Development
References:
Kamhi, A. (2014). Improving clinical practices for children with language and learning disorders. Language, Speech, and Hearing Services in Schools, 45(2), 92-103
Helpful Social Media Resources:
Creating a Comprehensive Speech Language Therapy Environment
 So you’ve completed a thorough evaluation of your student’s speech and language abilities and are in the process of creating goals and objectives to target in sessions. The problem is that many of the students on our caseloads present with pervasive deficits in many areas of language.
So you’ve completed a thorough evaluation of your student’s speech and language abilities and are in the process of creating goals and objectives to target in sessions. The problem is that many of the students on our caseloads present with pervasive deficits in many areas of language.
While it’s perfectly acceptable to target just a few goals per session in order to collect good data, both research and clinical experience indicate that addressing goals comprehensively and thematically (the whole system or multiple goals at once from the areas of content, form, and use) via contextual language intervention vs. in isolation (small parts such as prepositions, pronouns, etc.) will bring about the quickest change and more permanent results.

So how can that be done? Well, for significantly language impaired students it’s very important to integrate semantic language components as well as verbal reasoning tasks into sessions no matter what type of language activity you are working on (such as listening comprehension, auditory processing, social inferencing and so on). The important part is to make sure that the complexity of the task is commensurate with the student’s level of abilities.

Let’s say you are working on a fall themed lesson plans which include topics such as apples and pumpkins. As you are working on targeting different language goals, just throw in a few extra components to the session and ask the child to make, produce, explain, list, describe, identify, or interpret:
- Associations (“We just read a book about pumpkin: What goes with a pumpkin?”)
- Synonyms (“It said the leaves felt rough, what’s another word for rough?”)
- Antonyms (“what is the opposite of rough?”)
- Attributes 5+ (category, function, location, appearance, accessory/necessity, composition) (“Pretend I don’t know what a pumpkin is, tell me everything you can think of about a pumpkin”)
- Multiple Meaning Words (“The word felt has two meanings, it could mean _____ and it could also mean _______”)
- Definitions (“what is a pumpkin”)
- Compare and Contrast (“How are pumpkin and apple alike? How are they different?”)
- Idiomatic expressions (“Do you know what the phrase turn into a pumpkin means?” )
Ask ‘why’ and ‘how’ questions in order to start teaching the student how to justify, rationalize, evaluate, and make judgments regarding presented information (“Why do you think we plant pumpkins in the spring and not in the fall?”)
Don’t forget the inferencing and predicting questions in order to further develop the client’s verbal reasoning abilities (“What do you think will happen if no one picks up the apples from the ground?)
If possible attempt to integrate components of social language into the session such as ask client to relate to a character in a story, interpret the character’s feelings (“How do you think the girl felt when her sisters made fun of her pumpkin?”), ideas and thoughts, or just read nonverbal social cues such as body language or facial expressions of characters in pictures.
Select materials which are both multipurpose and reusable as well as applicable to a variety of therapy goals. For example, let’s take a simple seasonal word wall such as the (free) Fall Word Wall from TPT by Pocketful of Centers. Print it out in color, cut out the word strips and note how many therapy activities you can target for articulation, language, fluency, literacy and phonological awareness, etc.

Language:
Practice Categorization skills via convergent and divergent naming activities: Name Fall words, Name Halloween/Thanksgiving Words, How many trees whose leaves change color can you name?, how many vegetables and fruits do we harvest in the fall? etc.
Practice naming Associations: what goes with a witch (broom), what goes with a squirrel (acorn), etc
Practice providing Attributes via naming category, function, location, parts, size, shape, color, composition, as well as accessory/necessity. For example, (I see a pumpkin. It’s a fruit/vegetable that you can plant, grow and eat. You find it on a farm. It’s round and orange and is the size of a ball. Inside the pumpkin are seeds. You can carve it and make a jack o lantern out of it).
Practice providing Definitions: Tell me what a skeleton is. Tell me what a scarecrow is.
Practice naming Similarities and Differences among semantically related items: How are pumpkin and apple alike? How are they different?
Practice explaining Multiple Meaning words: What are some meanings of the word bat, witch, clown, etc?
Practice Complex Sentence Formulation: what happens in the fall? Make up a sentence with the words scarecrow and unless, make up a sentence with the words skeleton and however, etc

Phonological Awareness:
Practice Rhyming words (you can do discrimination and production activities): cat/bat/ trick/leaf/ rake/moon
Practice Syllable and Phoneme Segmentation (I am going to say a word (e.g., leaf, corn, scarecrow, etc) and I want you to clap one time for each syllable or sound I say)
Practice Isolation of initial, medial, and final phonemes in words ( e.g., What is the beginning/final sound in apple, hay, pumpkin etc?) What is the middle sound in rake etc?
Practice Initial and Final Syllable and Phoneme Deletion in Words (Say spider! Now say it without the der, what do you have left? Say witch, now say it without the /ch/ what is left; say corn, now say it without the /n/, what is left?)
Articulation/Fluency:
Practice production of select sounds/consonant clusters that you are working on or just production at word or sentence levels with those clients who just need a little bit more work in therapy increasing their intelligibility or sentence fluency.
So next time you are targeting your goals, see how you can integrate some of these suggestions into your data collection and let me know whether or not you’ve felt that it has enhanced your therapy sessions.
Happy Speeching! 
Helpful Resources:
- Creating Functional Therapy Plan
- Selecting Clinical Materials for Pediatric Therapy
- Vocabulary Development: Working With Disadvantaged Populations
- General Assessment and Treatment Start-Up Bundle
New Products for the 2017 Academic School Year for SLPs
September is quickly approaching and school-based speech language pathologists (SLPs) are preparing to go back to work. Many of them are looking to update their arsenal of speech and language materials for the upcoming academic school year.
With that in mind, I wanted to update my readers regarding all the new products I have recently created with a focus on assessment and treatment in speech language pathology. Continue reading New Products for the 2017 Academic School Year for SLPs
Back to School SLP Efficiency Bundles™
 September is practically here and many speech language pathologists (SLPs) are looking to efficiently prepare for assessing and treating a variety of clients on their caseloads.
September is practically here and many speech language pathologists (SLPs) are looking to efficiently prepare for assessing and treating a variety of clients on their caseloads.
With that in mind, a few years ago I created SLP Efficiency Bundles™, which are materials highly useful for SLPs working with pediatric clients. These materials are organized by areas of focus for efficient and effective screening, assessment, and treatment of speech and language disorders.
A. General Assessment and Treatment Start-Up Bundle contains 5 downloads for general speech language assessment and treatment planning and includes:
- Speech Language Assessment Checklist for a Preschool Child
- Speech Language Assessment Checklist for a School-Aged Child
- Creating a Functional Therapy Plan: Therapy Goals & SOAP Note Documentation
- Selecting Clinical Materials for Pediatric Therapy
- Types and Levels of Cues and Prompts in Speech Language Therapy
B. The Checklists Bundle contains 7 checklists relevant to screening and assessment in speech language pathology
- Speech Language Assessment Checklist for a Preschool Child 3:00-6:11 years of age
- Speech Language Assessment Checklist for a School-Aged Child 7:00-11:11 years of age
- Speech Language Assessment Checklist for Adolescents 12-18 years of age
- Language Processing Deficits (LPD) Checklist for School Aged Children 7:00-11:11 years of age
- Language Processing Deficits (LPD) Checklist for Preschool Children 3:00-6:11 years of age
- Social Pragmatic Deficits Checklist for School Aged Children 7:00-11:11 years of age
- Social Pragmatic Deficits Checklist for Preschool Children 3:00-6:11 years of age
C. Social Pragmatic Assessment and Treatment Bundle contains 6 downloads for social pragmatic assessment and treatment planning (from 18 months through school age) and includes:
- Recognizing the Warning Signs of Social Emotional Difficulties in Language Impaired Toddlers and Preschoolers
- Behavior Management Strategies for Speech Language Pathologists
- Social Pragmatic Deficits Checklist for School Aged Children
- Social Pragmatic Deficits Checklist for Preschool Children
- Assessing Social Pragmatic Skills of School Aged Children
- Treatment of Social Pragmatic Deficits in School Aged Children
D. Multicultural Assessment and Treatment Bundle contains 2 downloads relevant to assessment and treatment of bilingual/multicultural children
- Language Difference vs. Language Disorder: Assessment & Intervention Strategies for SLPs Working with Bilingual Children
- Impact of Cultural and Linguistic Variables On Speech-Language Services
E. Narrative Assessment Bundle contains 3 downloads relevant to narrative assessment
- Narrative Assessments of Preschool and School Aged Children
- Understanding Complex Sentences
- Vocabulary Development: Working with Disadvantaged Populations
F. Fetal Alcohol Spectrum Disorders Assessment and Treatment Bundle contains 3 downloads relevant to FASD assessment and treatment
- Orofacial Observations of At-Risk Children
- Fetal Alcohol Spectrum Disorder: An Overview of Deficits
- Speech Language Assessment and Treatment of Children With Alcohol Related Disorders
G. Psychiatric Disorders Bundle contains 7 downloads relevant to language assessment and treatment in psychiatrically impaired children
- Recognizing the Warning Signs of Social Emotional Difficulties in Language Impaired Toddlers and Preschoolers
- Social Pragmatic Deficits Checklist for School Aged Children
- Social Pragmatic Deficits Checklist for Preschool Children
- Assessing Social Skills in Children with Psychiatric Disturbances
- Improving Social Skills of Children with Psychiatric Disturbances
- Behavior Management Strategies for Speech Language Pathologists
- Differential Diagnosis Of ADHD In Speech Language Pathology
You can find these bundles on SALE in my online store by clicking on the individual bundle links above. You can also purchase these products individually in my online store by clicking HERE.
