
Differential Assessment and Treatment of Processing Disorders in Speech Language Pathology
 Today I am reviewing two products by Lindsey Swanson-Karol of the Word Nerd Speech Teach Blog related to the core curriculum: the Common Core Based Language Assessment as well as her Robot Phonological Awareness Pack.
Today I am reviewing two products by Lindsey Swanson-Karol of the Word Nerd Speech Teach Blog related to the core curriculum: the Common Core Based Language Assessment as well as her Robot Phonological Awareness Pack.
Those of you who follow my blog know that when I select materials, I always try to make sure that the materials are multipurpose, multi-functional, and curriculum embedded.
First up is the Common Core Based Language Assessment. This 14 page informal language assessment is based on the common core for K-5 grade in the areas of the curriculum relevant to speech-language pathology. Continue reading Focus on the common core
Today, after a long hiatus, I am continuing my series of blog posts on “Scholars Who do Not Receive Enough Mainstream Exposure” by summarizing select key points from Dr. Alan G. Kamhi’s 2004 article: “A Meme’s Eye View of Speech-Language Pathology“.

Some of you may be wondering: “Why is she reviewing an article that is more than a decade old? The answer is simple. It is just as relevant, if not more so today, as it was 12 years ago, when it first came out.
In this article, Dr. Kamhi, asks a provocative question: “Why do some terms, labels, ideas, and constructs [in the field of speech pathology] prevail whereas others fail to gain acceptance?“
He attempts to answer this question by explaining the vital role the concept of memes play in the evolution and spread of ideas.
A meme (shortened from the Greek mimeme to imitate) is “an idea, behavior, or style that spreads from person to person within a culture”. The term was originally coined by British evolutionary biologist Richard Dawkins in The Selfish Gene (1976) to explain the spread of ideas and cultural phenomena such as tunes, ideas, catchphrases, customs, etc.
‘Selfish’ in this case means that memes “care only about their own self-replication“. Consequently, “successful memes are those that get copied accurately (fidelity), have many copies (fecundity), and last a long time (longevity).” Therefore, “memes that are easy to understand, remember, and communicate to others” have the highest risk of survival and replication (pp. 105-106).
So what were some of the more successful memes which Dr. Kamhi identified in his article, which still persist more than a decade later?
Interestingly the losers of the “contest” were memes that contained the word language in it:
Dr. Kamhi further asserts that ‘language-based disorders have failed to become a recognizable learning problem in the community at large‘ (p.106).
So why are labels with the words ‘language’ NOT successful memes?
According to Dr. Kamhi that is because “language-based disorders must be difficult to understand, remember, and communicate to others“. Professional (SLP) explanations of what constitutes language are lengthy and complex (e.g., ASHA’s comprehensive definition) and as a result are not frequently applied in clinical practice, even when its aspects are familiar to SLPs.
Some scholars have suggested that the common practice of evaluating language with standardized language tools, restricts full understanding of the interactions of all of its domains (“within larger sociocultural context“) because they only examine isolated aspects of language. (Apel, 1999)
Dr. Kamhi, in turn explains this within the construct of the memetic theory: namely “simple constructs are more likely to replicate than complex ones.” In other words: “even professionals who understand language may have difficulty communicating its meaning to others and applying this meaning to clinical practice” (p. 107).
Let’s talk about the parents who are interested in learning the root-cause of their child’s difficulty learning and using language. Based on specific child’s genetic and developmental background as well as presenting difficulties, an educated clinician can explain to the parent the multifactorial nature of their child’s deficits.
However, these informed but frequently complex explanations are certainly in no way simplistic. As a result, many parents will still attempt to seek other professionals who can readily provide them with a “straightforward explanation” of their child’s difficulty. Since parents are “ultimately interested in finding the most effective and efficient treatment for their children” it makes sense to believe/hope that “the professional who knows the cause of the problem will also know the most effective way to treat it“(p. 107).
This brings us back to the concept of successful memes such as Auditory Processing Disorder (C/APD) as well as Sensory Processing Disorder (SPD) as isolated diagnoses.
Here are just some of the reasons behind their success:
For more information on why APD and SPD are not valid stand-alone diagnoses please see HERE and HERE respectively.
A note on the lack of success of “phonological” memes:
Let’s talk about MEMEPLEXES (Blackmore, 1999) or what occurs when “nonprofessionals think they know how children learn language and the factors that affect language learning“ (Kamhi, 2004, p.108).
A memplex is a group of memes, which become much more memorable to individuals (can replicate more efficiently) as a team vs. in isolation.
Why is APD Memeplex So Appealing?
According to Dr. Kamhi, if one believes that ‘a) sounds are the building blocks of speech and language and (b) children learn to talk by stringing together sounds and constructing meanings out of strings of sounds’ (both wrong assumptions) then its quite a simple leap to make with respect to the following fallacies:

For more detailed information, why the above is incorrect, click: HERE
On the success of the Dyslexia Meme:
For more detailed information, why the above is far too simplistic of an explanation, click: HERE and HERE.
Final Thoughts:
As humans we engage in transmission of ideas (good and bad) on constant basis. The popularity of powerful social media tools such as Facebook and Twitter ensure their instantaneous and far reaching delivery and impact. However, “our processing limitations, cultural biases, personal preferences, and human nature make us more susceptible to certain ideas than to others (p. 110).”
As professionals it is important that we use evidence based practices and the latest research to evaluate all claims pertaining to assessment and treatment of language based disorders. However, as Dr. Kamhi points out (p.110):
While these delays may play a negligible role when it comes to scientific research, they pose a significant problem for parents, teachers and health professionals who are seeking to effectively assist these youngsters on daily basis. Furthermore, even when select memes such as APD are beneficial because they allow for a delivery of services to a student who may otherwise be ineligible to receive them, erroneous intervention recommendations (e.g., working on isolated auditory discrimination skills) may further delay the delivery of appropriate and targeted intervention services.
So what are SLPs to do in the presence of persistent erroneous memes?
“Spread our language-based memes to all who will listen” (Kamhi, 2004, 110) of course! Since we are the professionals whose job is to treat any difficulties involving words. Consequently, our scope of practice certainly includes assessment, diagnosis and treatment of children and adults with speaking, listening, reading, writing, and spelling difficulties.
As for myself, I intend to start that task right now by hitting the ‘publish’ button on this post!

References:
Kamhi, A. (2004). A meme’s eye view of speech-language pathology. [PDF] Language, Speech, and Hearing Services in Schools, 35, 105-112.
 Back to school time is just around the corner and if your job is anything like mine then you are getting ready to perform a number of speech language screenings and assessments after the kids get back to school in September. In order to optimize the assessment process I’ve created a number of checklists and forms for my (and your convenience). They allow for quick and efficient determination of whether the preschool/school age monolingual/bilingual student in question requires any speech language services including: screening, assessment, future follow-up, or on-going monitoring. Please note that for bilingual students it is recommended that parents mark whether the child presents with deficits in one language or in both on the checklists (e.g., mark R, E, or B – Russian, English or both).
Back to school time is just around the corner and if your job is anything like mine then you are getting ready to perform a number of speech language screenings and assessments after the kids get back to school in September. In order to optimize the assessment process I’ve created a number of checklists and forms for my (and your convenience). They allow for quick and efficient determination of whether the preschool/school age monolingual/bilingual student in question requires any speech language services including: screening, assessment, future follow-up, or on-going monitoring. Please note that for bilingual students it is recommended that parents mark whether the child presents with deficits in one language or in both on the checklists (e.g., mark R, E, or B – Russian, English or both).
Speech Language Assessment Checklist For A Preschool Child is a 9 page guide created to assist speech language pathologists in the decision making process of how to select assessment instruments and prioritize assessment for preschool children 3:00-5:11 years of age. The goal is to eliminate administration of unnecessary or irrelevant tests and focus on the administration of instruments directly targeting the areas of difficulty that the child presents with.
It contains:
Checklist Target Areas:
Speech Language Assessment Checklist For A School-Aged Child is a 12 page guide created to assist speech language pathologists in the decision making process of how to select assessment instruments and prioritize assessment for school age children. The goal is to eliminate administration of unnecessary or irrelevant tests and focus on the administration of instruments directly targeting the areas of difficulty that the child presents with.
It contains:
Checklist Target Areas:
Auditory Processing Deficits Checklist for School Aged Children was created to assist speech language pathologists (SLPs) with figuring out whether the student presents with auditory processing deficits which require further follow up (e.g., screening, comprehensive assessment). The SLP should provide this form to both teacher and caregiver/s to fill out to ensure that the deficit areas are consistent across all settings and people.
Checklist Categories:
General Organizational Abilities
Social Pragmatic Deficits Checklist for School Aged Children was created to assist speech language pathologists (SLPs) with figuring out whether the student presents with social pragmatic language deficits which require further follow up (e.g., assessment). The SLP should provide this form to both teacher and caregiver/s to fill out to ensure that the deficit areas are consistent across all settings and people.
Checklist Categories:
You can find these products by clicking on the individual links above. You can also find many other educational products relevant to assessment and treatment in speech language pathology in my online store by clicking HERE.

Happy and successful new school year everyone!
 One common difficulty our “higher functioning” (refers to subjective notion of ‘perceived’ functioning in school setting only) language impaired students with social communication and executive function difficulties present with – is lack of insight into own strengths and weaknesses.
One common difficulty our “higher functioning” (refers to subjective notion of ‘perceived’ functioning in school setting only) language impaired students with social communication and executive function difficulties present with – is lack of insight into own strengths and weaknesses.
Yet insight is a very important skill, which most typically developing students exhibit without consciously thinking about it. Having insight allows students to review work for errors, compensate for any perceived weaknesses effectively, and succeed with efficient juggling of academic workload.
In contrast, lack of insight in students with language deficits further compounds their difficulties, as they lack realization into own weaknesses and as a result are unable to effectively compensate for them.
That is why I started to explicitly teach the students on my caseload in both psychiatric hospital and private practice the concept of insight.
Now some of you may have some legitimate concerns. You may ask: “How can one teach such an abstract concept to students who are already impaired in their comprehension of language?” The answer to that is – I teach this concept through a series of concrete steps as well as through the introduction of abstract definitions, simplified for the purpose of my sessions into concrete terms.
Furthermore, it is important to understand that the acquisition of “insight” cannot be accomplished in one or even several sessions. Rather after this concept is introduced and the related vocabulary has been ‘internalized’ by the student, thematic therapy sessions can be used to continue the acquisition of “insight” for months and even years to come.

How do we begin?
When I first started teaching this concept I used to explain the terminology related to “insight” verbally to students. However, as my own ‘insight’ developed in response to the students’ performance, I created a product to assist them with the acquisition of insight (See HERE).
Intended Audiences:

This thematic 10 page packet targets the development of “insight” in students with average IQ, 8+ years of age, presenting with social pragmatic and executive function difficulties.
The packet contains 1 page text explaining the concept of insight to students.
It also contains 11 Tier II vocabulary words relevant to the discussion of insight and their simplified definitions. The words were selected based on course curriculum standards for several grade levels (fourth through seventh) due to their wide usage in a variety of subjects (social studies, science, math, etc.)
Language activities in this packet include:
And now a few words regarding the lesson structure…
I introduce the concept of “insight” to clients by writing down the word and asking them to identify its parts: ‘in‘ and ‘sight‘. Depending on the student’s level of abilities I either get to the students to explain it to me or explain it myself that it is a compound word made up of two other words.
I then ask the students to interpret what the word could potentially mean. After I hear their responses I either confirm the correct one or end up explaining that this word refers to “looking into one’s brain” for answers related to how well someone understands information.
I have the students read the text located on the first page of my packet going over the concept of insight and some of its associated vocabulary words. I ask the students to tell me the main idea of each paragraph as well as answer questions regarding supporting text details.
Once I am confident that the students have a fairly good grasp of the presented text I move on to the definitions page. There are actually two definition pages in the lesson: one at the beginning and one at the end of the packet. The first definitions page also contains word meaning and what parts of speech the definitions belong to. The definition page at the end of the packet contains only the targeted words. It is now the students responsibility to write down the definition of all the vocabulary words and phrases in order for me to see how well they remember the meanings of pertinent words.
The packet also includes comprehension questions, a section on sentence construction several morphological awareness activities, a crossword puzzle and a self-reflection page.
The final activity in the packet requires the student to judge their own work performance during this activity. I ask students questions such as:
If a student responds “I know I did well because I understood everything”, I typically ask them to prove their comprehension to me, verbally. Here the goal is to have the student provide concrete verbal examples supporting their insight of their performance.
This may include statements such as:
As mentioned above this activity is only the beginning. After I ensure that the students have a decent grasp of this concept I continue working on it indirectly by having the students continuously judge their own performance on a variety of other therapy related activities and assignments.
You can find the complete packet on teaching “insight” in my online store (HERE). Also, stay tuned for Part II of this series, which will describe how to continue solidifying the concept of “insight” in the context of therapy sessions for students with social pragmatic and executive function deficits.
Helpful Smart Speech Resources:
 Our ability to recognize our own and other people’s emotions, distinguish between and correctly identify different feelings, as well as use that information to guide our thinking and behavior is called Emotional Intelligence (EI) (Salovey, et al, 2008).
Our ability to recognize our own and other people’s emotions, distinguish between and correctly identify different feelings, as well as use that information to guide our thinking and behavior is called Emotional Intelligence (EI) (Salovey, et al, 2008).
EI encompasses dual areas of: emotion understanding, which is an awareness and comprehension of one’s and others emotions (Harris, 2008) and emotion regulation, which are internal and external strategies people use to regulate emotions (Thompson, 1994).
Many students with social communication challenges experience problems with all aspects of EI, including the perception, comprehension, and regulation of emotions (Brinton & Fujiki, 2012).
A number of recent studies have found that children with language impairments also present with impaired emotional intelligence including impaired perception of facial expressions (Spackman, Fujiki, Brinton, Nelson, & Allen, 2005), prosodic emotions (Fujiki, Spackman, Brinton, & Illig, 2008) as well as abstract emotion comprehension (Ford & Milosky, 2003).

Children with impaired emotional intelligence will experience numerous difficulties during social interactions due to their difficulty interpreting emotional cues of others (Cloward, 2012). These may include but not be limited to active participation in cooperative activities, as well as full/competent interactions during group tasks (Brinton, Fujiki, & Powell, 1997)
Many students with social pragmatic deficits and language impairments are taught to recognize emotional states as part of their therapy goals. However, the provided experience frequently does not go beyond the recognition of the requisite “happy”, “mad”, “sad” emotions. At times, I even see written blurbs from others therapists, which state that “the student has mastered the goals of emotion recognition”. However, when probed further it appears that the student had merely mastered the basic spectrum of simple emotional states, which places the student at a distinct disadvantage as compared to typically developing peers who are capable of recognition and awareness of a myriad of complex emotional states.

That is why I developed a product to target abstract emotional states comprehension in children with language impairments and social communication disorders. “Gauging Moods and Interpreting Abstract Emotional States: A Perspective Taking Activity Packet” is a social pragmatic photo/question set, intended for children 7+ years of age, who present with difficulty recognizing abstract emotional states of others (beyond the “happy, mad, sad” option) as well as appropriately gauging their moods.
Many sets contain additional short stories with questions that focus on making inferencing, critical thinking as well as interpersonal negotiation skills. Select sets require the students to create their own stories with a focus on the reasons why the person in the photograph might be feeling what s/he are feeling.

There are on average 12-15 questions per each photo. Each page contains a photograph of a person feeling a particular emotion. After the student is presented with the photograph, they are asked a number of questions pertaining to the recognition of the person’s emotions, mood, the reason behind the emotion they are experiencing as well as what they could be potentially thinking at the moment. Students are also asked to act out the depicted emotion they use of mirror.
Activities also include naming or finding (in a thesaurus or online) the synonyms and antonyms of a particular word in order to increase students’ vocabulary knowledge. A comprehensive two page “emotions word bank” is included in the last two pages of the packet to assist the students with the synonym/antonym selection, in the absence of a thesaurus or online access.

Students are also asked to use a target word in a complex sentence containing an adverbial (pre-chosen for them) as well as to identify a particular word or phrase associated with the photo or the described story situation.
Since many students with social pragmatic language deficits present with difficulty determining a person’s age (and prefer to relate to either younger or older individuals who are perceived to be “less judgmental of their difficulties”), this concept is also explicitly targeted in the packet.
This activity is suitable for both individual therapy sessions as well as group work. In addition to its social pragmatic component is also intended to increase vocabulary knowledge and use as well as sentence length of children with language impairments.
Intended Audiences:
Areas covered in this packet:
This activity is suitable for both individual therapy sessions as well as group work. In addition to its social pragmatic component is also intended to increase vocabulary knowledge and use as well as sentence length of children with language impairments. You can find it in my online store (HERE).
Helpful Smart Speech Resources:
References:
 Today I am very exited to start DAY 1 of my Birthday Month Giveaways by raffling off a giveaway by Figuratively Speeching SLP, which is a book companion to Lucille Colandro’s “There was an old lady who swallowed some leaves”.
Today I am very exited to start DAY 1 of my Birthday Month Giveaways by raffling off a giveaway by Figuratively Speeching SLP, which is a book companion to Lucille Colandro’s “There was an old lady who swallowed some leaves”.
This is a lovely 33 page supplemental packet to the book which includes a variety of activities aimed at improving the student’s auditory processing (following one, two-step directions,and conditional directions), listening comprehension (story questions), vocabulary knowledge and use, sequencing ability, story retelling ability, phonological awareness skills (identifying the first sound in vocabulary words), articulation abilities (word lists and homework pages) and much much more. You can find this product in her TPT store by clicking HERE or you can enter my one day giveaway for a chance to win.
Do you accept insurance reimbursement?
Unfortunately we do not. We are an out of network insurance provider.
How do I submit for out of network speech therapy reimbursement?
You will be provided with an invoice to submit to your insurance company. It will contain the necessary information including: diagnosis and treatment codes, session times, fees paid, description of services provided, as well as pertinent practice information (tax id, license number, etc). We will also provide you with assessment and therapy progress reports to submit to your insurance company along with the invoice.
What are your assessment fees?
Our assessments are varied and highly individualized. Assessment fees are based on our hourly rates and are dependent on a number of factors (e.g., face to face time spent with the client, report writing time, etc). Prior to assessment parents are asked to fill out detailed intake and referral forms for their child in order to determine which testing instruments need to be administered.
Do you conduct in home assessments and treatment?
Unfortunately due to time constraints all services are provided on-site only.
What are your hours of operation?
We try to accommodate all our busy customers by offering weekday afternoon and evening, as well as weekend hours.
How do I initiate assessment and/or therapy?
Please call us for a free consultation at the number listed on our website. Once we determine that our services are right for your child, you will receive a password to download the appropriate forms and releases.
How long do your assessments typically last?
Comprehensive assessments for younger children (infants, toddlers, preschoolers and early school age children) typically last between 2-3 hours and are performed during 1 visit. Comprehensive assessments for older school age children may last between 4-5 hours and are usually broken into 2 sessions over a period of several days. All assessments are highly individualized and are dependent on the client’s unique needs (e.g., is assessment needed to qualify the child for in district school therapy services, are parents seeking an independent evaluation to be used in a court case, etc)
What can I expect as a result of my child’s speech language assessment?
Two weeks subsequent to the last assessment date you will receive a comprehensive speech language report detailing your child’s performance on administered formal and informal testing. It will contain performance scores (if applicable), detailed descriptive summary of performance strengths and weaknesses, impressions, recommendations, referral for additional professional consultations (if needed), treatment goals and objectives as well as suggested remediation methods, techniques, and strategies.
If you perform the assessment, but we are unable to come to you for treatment, what options are available to us?
We offer comprehensive assessments and reassessments for out of state and out of county clients. Our subsequent recommendations within the body of the report are very detailed, supported by the latest evidenced based research, and are very easy to follow. Out of state comprehensive re/assessments are often requested by parents due to the absence of qualified and highly trained professionals in their specific geographic area. Such assessments are especially relevant for a select group of older internationally adopted OR functionally bilingual Russian speaking children with complex diagnoses/disabilities (Fetal Alcohol Spectrum Disorder, Mental Retardation, Genetic Disorders, Autistic Spectrum Disorders, etc), who attain limited success in therapeutic setting despite years and years of therapeutic intervention provision.
Other times we are asked to perform assessments with children who fail to qualify for intervention services within their state school system, due to limited assessment practices (therapist may administer select subtests from a general language test but does not assess the child’s social pragmatic skills, auditory processing skills, executive function, or critical thinking abilities), despite the child presenting with a number of profound linguistic, critical thinking, and social pragmatic deficits.
We perform the necessary testing based on presenting symptomology and then we’ll provide you with a comprehensive report detailing the subsequent requirements for treatment/referrals (if needed), which other therapists can then implement in the child’s home state/county.
What if another therapist conducted the assessment do I still have to repeat the evaluation process?
In most circumstances testing will only need to be repeated if it’s significantly outdated. Typically if the assessment was done within the past year, and the results are still accurately representative of the child’s present performance, therapy may be initiated immediately. However, there may be a number of instances when the clinician may suggest a reassessment. Below are some examples:
· Testing report is outdated/not accurately representative of child’s present performance
· Testing instruments used were outdated/no longer relevant to the child’s present needs
· Testing was not comprehensive enough (child is scoring within normal limits on a specific test but still presents with significant deficits in other areas)
In such instances a partial/full reassessment may be recommended in the context of initial therapy sessions, in order to establish a baseline for intervention provision.
What is the average therapy frequency and duration?
Average therapy frequency is 1 time per week for a duration of 1 hour. Select clients receive higher therapy frequency and lower therapy duration; still others come in on biweekly or monthly basis to maintain skill level/abilities.
What type of service delivery do you provide?
Vast majority of sessions are provided on individual basis. Group sessions are subject to availability. Peer tutoring/coaching is often implemented when working on social language skills.
How long will my child attend speech therapy?
Therapy duration is dependent on a number of factors:
· Type and level of impairment (clients with significant disabilities such as mental retardation or autism spectrum disorders receive ongoing support and treatment vs. clients with articulation disorders, who are in therapy for a short number of weeks/months)
· Presence of maintaining factors (e.g., psychiatric diagnosis, other structural/functional deficits)
· Existence of additional support services (is the child receiving school based therapy, resource room, reading recovery, etc)
· Parental involvement (supervision of homework, reinforcement of current skills)
· Client motivation
How do you determine when the child is ready to be discharged from therapy services?
Client progress is charted on an ongoing basis. Frequent reassessments of deficit areas are administered during the course of treatment.
Additional Links:
Please see the following FAQ links from American Speech-Language-Hearing Association (ASHA) for further information:
Speech and Language Disorders in the School Setting: http://www.asha.org/
 So you’ve completed a thorough evaluation of your student’s speech and language abilities and are in the process of creating goals and objectives to target in sessions. The problem is that many of the students on our caseloads present with pervasive deficits in many areas of language.
So you’ve completed a thorough evaluation of your student’s speech and language abilities and are in the process of creating goals and objectives to target in sessions. The problem is that many of the students on our caseloads present with pervasive deficits in many areas of language.
While it’s perfectly acceptable to target just a few goals per session in order to collect good data, both research and clinical experience indicate that addressing goals comprehensively and thematically (the whole system or multiple goals at once from the areas of content, form, and use) via contextual language intervention vs. in isolation (small parts such as prepositions, pronouns, etc.) will bring about the quickest change and more permanent results.

So how can that be done? Well, for significantly language impaired students it’s very important to integrate semantic language components as well as verbal reasoning tasks into sessions no matter what type of language activity you are working on (such as listening comprehension, auditory processing, social inferencing and so on). The important part is to make sure that the complexity of the task is commensurate with the student’s level of abilities.

Let’s say you are working on a fall themed lesson plans which include topics such as apples and pumpkins. As you are working on targeting different language goals, just throw in a few extra components to the session and ask the child to make, produce, explain, list, describe, identify, or interpret:
Ask ‘why’ and ‘how’ questions in order to start teaching the student how to justify, rationalize, evaluate, and make judgments regarding presented information (“Why do you think we plant pumpkins in the spring and not in the fall?”)
Don’t forget the inferencing and predicting questions in order to further develop the client’s verbal reasoning abilities (“What do you think will happen if no one picks up the apples from the ground?)
If possible attempt to integrate components of social language into the session such as ask client to relate to a character in a story, interpret the character’s feelings (“How do you think the girl felt when her sisters made fun of her pumpkin?”), ideas and thoughts, or just read nonverbal social cues such as body language or facial expressions of characters in pictures.
Select materials which are both multipurpose and reusable as well as applicable to a variety of therapy goals. For example, let’s take a simple seasonal word wall such as the (free) Fall Word Wall from TPT by Pocketful of Centers. Print it out in color, cut out the word strips and note how many therapy activities you can target for articulation, language, fluency, literacy and phonological awareness, etc.

Language:
Practice Categorization skills via convergent and divergent naming activities: Name Fall words, Name Halloween/Thanksgiving Words, How many trees whose leaves change color can you name?, how many vegetables and fruits do we harvest in the fall? etc.
Practice naming Associations: what goes with a witch (broom), what goes with a squirrel (acorn), etc
Practice providing Attributes via naming category, function, location, parts, size, shape, color, composition, as well as accessory/necessity. For example, (I see a pumpkin. It’s a fruit/vegetable that you can plant, grow and eat. You find it on a farm. It’s round and orange and is the size of a ball. Inside the pumpkin are seeds. You can carve it and make a jack o lantern out of it).
Practice providing Definitions: Tell me what a skeleton is. Tell me what a scarecrow is.
Practice naming Similarities and Differences among semantically related items: How are pumpkin and apple alike? How are they different?
Practice explaining Multiple Meaning words: What are some meanings of the word bat, witch, clown, etc?
Practice Complex Sentence Formulation: what happens in the fall? Make up a sentence with the words scarecrow and unless, make up a sentence with the words skeleton and however, etc

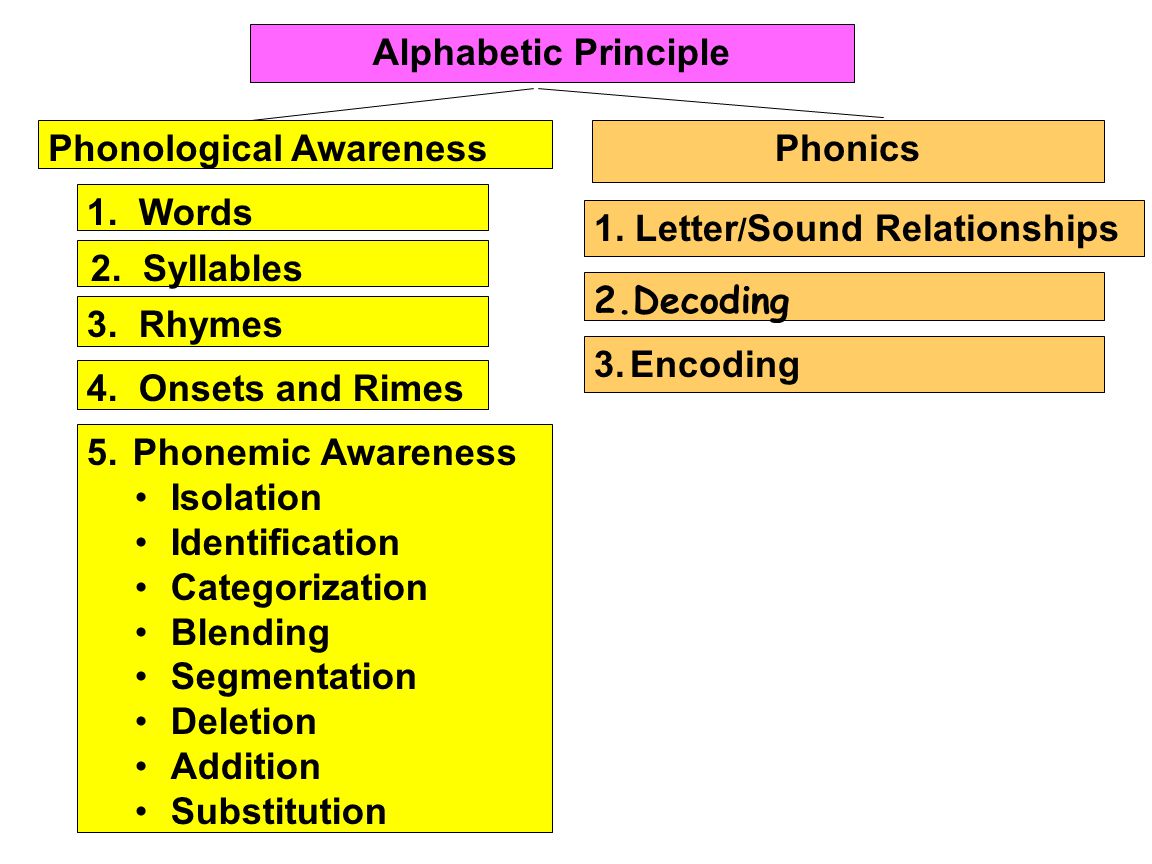
Phonological Awareness:
Practice Rhyming words (you can do discrimination and production activities): cat/bat/ trick/leaf/ rake/moon
Practice Syllable and Phoneme Segmentation (I am going to say a word (e.g., leaf, corn, scarecrow, etc) and I want you to clap one time for each syllable or sound I say)
Practice Isolation of initial, medial, and final phonemes in words ( e.g., What is the beginning/final sound in apple, hay, pumpkin etc?) What is the middle sound in rake etc?
Practice Initial and Final Syllable and Phoneme Deletion in Words (Say spider! Now say it without the der, what do you have left? Say witch, now say it without the /ch/ what is left; say corn, now say it without the /n/, what is left?)
Articulation/Fluency:
Practice production of select sounds/consonant clusters that you are working on or just production at word or sentence levels with those clients who just need a little bit more work in therapy increasing their intelligibility or sentence fluency.
So next time you are targeting your goals, see how you can integrate some of these suggestions into your data collection and let me know whether or not you’ve felt that it has enhanced your therapy sessions.
Happy Speeching! 
Helpful Resources:
![]() Several years ago I began blogging on the subject of independent assessments in speech pathology. First, I wrote a post entitled “Special Education Disputes and Comprehensive Language Testing: What Parents, Attorneys, and Advocates Need to Know“, in which I used 4 different scenarios to illustrate the importance of comprehensive language evaluations for children with subtle language and learning needs. Then I wrote about: “What Makes an Independent Speech-Language-Literacy Evaluation a GOOD Evaluation?” in order to elucidate on what actually constitutes a good independent comprehensive assessment. Continue reading Neuropsychological or Language/Literacy: Which Assessment is Right for My Child?
Several years ago I began blogging on the subject of independent assessments in speech pathology. First, I wrote a post entitled “Special Education Disputes and Comprehensive Language Testing: What Parents, Attorneys, and Advocates Need to Know“, in which I used 4 different scenarios to illustrate the importance of comprehensive language evaluations for children with subtle language and learning needs. Then I wrote about: “What Makes an Independent Speech-Language-Literacy Evaluation a GOOD Evaluation?” in order to elucidate on what actually constitutes a good independent comprehensive assessment. Continue reading Neuropsychological or Language/Literacy: Which Assessment is Right for My Child?