
Recently I began writing a series of posts on the topic of comprehensive assessment of dyslexia.
In part I of my post (HERE), I discussed common dyslexia myths as well as general language testing as a starting point in the dyslexia testing battery.
In part II I detailed the next two steps in dyslexia assessment: phonological awareness and word fluency testing (HERE).
Today I would like to discuss part III of comprehensive dyslexia assessment, which discusses reading fluency and reading comprehension testing.
Let’s begin with reading fluency testing, which assesses the students’ ability to read word lists or short paragraphs with appropriate speed and accuracy. Here we are looking for how many words the student can accurately read per minute orally and/or silently (see several examples of fluency rates below).

Research indicates that oral reading fluency (ORF) on passages is more strongly related to reading comprehension than ORF on word lists. This is an important factor which needs to be considered when it comes to oral fluency test selection.
Oral reading fluency tests are significant for a number of reasons. Firstly, they allow us to identify students with impaired reading accuracy. Secondly, they allow us to identify students who can decode words with relative accuracy but who cannot comprehend what they read due to significantly decreased reading speed. When you ask such children: “What did you read about?” They will frequently respond: “I don’t remember because I was so focused on reading the words correctly.”
One example of a popular oral reading fluency test (employing reading passages) is the Gray Oral Reading Tests-5 (GORT-5). It yields the scores on the student’s:
- Rate
- Accuracy
- Fluency
- Comprehension
- Oral Reading Index (a composite score based on Fluency and Comprehension scaled scores)
Another types of reading fluency tests are tests of silent reading fluency. Assessments of silent reading fluency can at selectively useful for identifying older students with reading difficulties and monitoring their progress. One obvious advantage to silent reading tests is that they can be administered in group setting to multiple students at once and generally takes just few minutes to administer, which is significantly less then oral reading measures take to be administered to individual students.
Below are a several examples of silent reading tests/subtests.
 The Test of Silent Word Reading Fluency (TOSWRF-2) presents students with rows of words, ordered by reading difficulty without spaces (e.g., dimhowfigblue). Students are given 3 minutes to draw a line between the boundaries of as many words as possible (e.g., dim/how/fig/blue).
The Test of Silent Word Reading Fluency (TOSWRF-2) presents students with rows of words, ordered by reading difficulty without spaces (e.g., dimhowfigblue). Students are given 3 minutes to draw a line between the boundaries of as many words as possible (e.g., dim/how/fig/blue).
The Test of Silent Contextual Reading Fluency (TOSCRF-2) presents students with text passages with all words printed in uppercase letters with no separations between words and no punctuation or spaces between sentences and asks them to use dashes to separate words in a 3 minute period.
Similar to the TOSCRF-2, the Contextual Fluency subtest of the Test of Reading Comprehension – Fourth Edition (TORC-4) measures the student’s ability to recognize individual words in a series of passages (taken from the TORC-4′s Text Comprehension subtest) in a period of 3 minutes. Each passage, printed in uppercase letters without punctuation or spaces between words, becomes progressively more difficult in content, vocabulary, and grammar. As students read the segments, they draw a line between as many words as they can in the time allotted. (E.g., THE|LITTLE|DOG|JUMPED|HIGH)
However, it is important to note oral reading fluency is a better predictor of reading comprehension than is silent reading fluency for younger students (early elementary age). In contrast, silent reading measures are more strongly related to reading comprehension in middle school (e.g., grades 6-8) but only for skilled vs. average readers, which is why oral reading fluency measures are probably much better predictors of deficits in this area in children with suspected reading disabilities.
Now let’s move on to the reading comprehension testing, which is an integral component for any dyslexia testing battery. Unfortunately, it is also the most trickiest. Here’s why.
Many children with reading difficulties will be able to read and comprehend short paragraphs containing factual information of decreased complexity. However, this will change dramatically when it comes to the comprehension of longer, more complex, and increasingly abstract age-level text. While a number of tests do assess reading comprehension, none of them truly adequately assess the students ability to comprehend abstract information.
For example, on the Reading Comprehension subtest of the CELF-5, students are allowed to keep the text and refer to it when answering questions. Such option will inflate the students scores and not provide an accurate idea of their comprehension abilities.
To continue, the GORT-5 contains reading comprehension passages, which the students need to answer after the stimuli booklet has been removed from them. However, the passages are far more simplistic then the academic texts the students need to comprehend on daily basis, so the students may do well on this test yet still continue to present with significant comprehension deficits.
Similar could be said for the text comprehension components of major educational testing batteries such as the Woodcock Johnson IV: Passage Comprehension subtest, which gives the student sentences with a missing word, and the student is asked to orally provide the word. However, filling-in a missing word does not text comprehension make.
Likewise, the Wechsler Individual Achievement Test®-Fourth Edition (WIAT-IV), Reading Comprehension subtest is very similar to the CELF-5. Student is asked to read a passage and answer questions by referring back to the text. However, just because a student can look up the answers in text does not mean that they actually understand the text.
So what could be done to accurately assess the student’s ability to comprehend abstract grade level text? My recommendation is to go informal. Select grade-level passages from the student’s curriculum pertaining to science, social studies, geography, etc. vs. language arts (which tends to be more simplistic) and ask the student to read them and answer factual questions regarding supporting details as well as non factual questions relevant to main ideas and implied messages.
That’s it for today’s post! Click (HERE) for part IV of this series which will discuss components of Writing and Spelling testing.
 In mid-2014, I purchased the
In mid-2014, I purchased the  Errors on this subtest can result due to pragmatic, semantic or syntactic errors. With respect to pragmatics errors can result due to illogical, nonsensical, vague or incomplete sentences as well as due to sentence formulation which does not take into account presented scenes. With respect to semantics errors can result due to missing or misused target words as well as due to vague, incorrect or misused verbiage. With respect to syntax errors can result due to use of sentence fragments, morphological misuse of target words (changing word forms) as well as syntact deviations on non-target words.
Errors on this subtest can result due to pragmatic, semantic or syntactic errors. With respect to pragmatics errors can result due to illogical, nonsensical, vague or incomplete sentences as well as due to sentence formulation which does not take into account presented scenes. With respect to semantics errors can result due to missing or misused target words as well as due to vague, incorrect or misused verbiage. With respect to syntax errors can result due to use of sentence fragments, morphological misuse of target words (changing word forms) as well as syntact deviations on non-target words. What I am concerned about:
What I am concerned about: 
 Today I want to talk treatment. That thing that we need to plan for as we are doing our assessments. But are we starting our treatments the right way? The answer may surprise you. I often see SLPs phrasing questions regarding treatment the following way: “I have a student diagnosed with ____ (insert disorder here). What is everyone using (program/app/materials) during therapy sessions to address ___ diagnosis?”
Today I want to talk treatment. That thing that we need to plan for as we are doing our assessments. But are we starting our treatments the right way? The answer may surprise you. I often see SLPs phrasing questions regarding treatment the following way: “I have a student diagnosed with ____ (insert disorder here). What is everyone using (program/app/materials) during therapy sessions to address ___ diagnosis?” There could be endless variations of how deficits manifest in poor readers. Is it aspects of phonological awareness, phonics, morphology, etc. What combination of deficits is preventing the child from becoming a good reader?
There could be endless variations of how deficits manifest in poor readers. Is it aspects of phonological awareness, phonics, morphology, etc. What combination of deficits is preventing the child from becoming a good reader?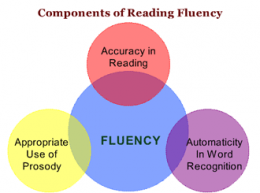 Reading Fluency: “LG’s reading fluency during this task was judged to be significantly affected by excessive speed, inappropriate pausing, word misreadings, choppy prosody, as well as inefficient word attack skills. While she was able to limitedly utilize the phonetic spelling of unfamiliar words (e.g., __) provided to her in parenthesis next to the word (which she initially misread as ‘__’), she exhibited limited use of metalinguistic strategies (e.g., pre-scanning sentences to aid text comprehension, self-correcting to ensure that the read words made sense in the context of the sentence, etc.), when reading the provided passage. To illustrate, during the reading of the text, LG was observed to frequently (at least 3 times) lose her place and skip entire lines of text without any attempts at self-correction. At times she was observed to read the same word a number of different ways (e.g., read ‘soup’ as ‘soup’ then as ‘soap’, ‘roots’ as ‘roofs’ then as ‘roots’, etc.) without attempting to self-correct. LG’s oral reading rate was also observed to be impaired for her age/grade levels. Her prosody was significantly adversely affected due to lack of adequate pausing for punctuation marks (e.g., periods, commas, etc.). Instead, she paused during text reading only when he could not decode select words in the text. Though, LG was able to read 70 words per minute, which was judged to be grossly commensurate with grade-level, out of these 70 words she skipped 2 entire lines of text, invented an entire line of text, as well as made 4 decoding errors and 6 inappropriate pauses.”
Reading Fluency: “LG’s reading fluency during this task was judged to be significantly affected by excessive speed, inappropriate pausing, word misreadings, choppy prosody, as well as inefficient word attack skills. While she was able to limitedly utilize the phonetic spelling of unfamiliar words (e.g., __) provided to her in parenthesis next to the word (which she initially misread as ‘__’), she exhibited limited use of metalinguistic strategies (e.g., pre-scanning sentences to aid text comprehension, self-correcting to ensure that the read words made sense in the context of the sentence, etc.), when reading the provided passage. To illustrate, during the reading of the text, LG was observed to frequently (at least 3 times) lose her place and skip entire lines of text without any attempts at self-correction. At times she was observed to read the same word a number of different ways (e.g., read ‘soup’ as ‘soup’ then as ‘soap’, ‘roots’ as ‘roofs’ then as ‘roots’, etc.) without attempting to self-correct. LG’s oral reading rate was also observed to be impaired for her age/grade levels. Her prosody was significantly adversely affected due to lack of adequate pausing for punctuation marks (e.g., periods, commas, etc.). Instead, she paused during text reading only when he could not decode select words in the text. Though, LG was able to read 70 words per minute, which was judged to be grossly commensurate with grade-level, out of these 70 words she skipped 2 entire lines of text, invented an entire line of text, as well as made 4 decoding errors and 6 inappropriate pauses.” Those of you familiar with my blog, know that a number of my posts take on a form of extended responses to posts and comments on social media which deal with certain questionable speech pathology trends and ongoing issues (e.g., controversial diagnostic labels, questionable recommendations, non-evidence based practices, etc.). So, today, I’d like to talk about sweeping general recommendations as pertaining to literacy interventions.
Those of you familiar with my blog, know that a number of my posts take on a form of extended responses to posts and comments on social media which deal with certain questionable speech pathology trends and ongoing issues (e.g., controversial diagnostic labels, questionable recommendations, non-evidence based practices, etc.). So, today, I’d like to talk about sweeping general recommendations as pertaining to literacy interventions.  The end of the school year is almost near. Soon many of our clients with language and literacy difficulties will be going on summer vacation and enjoying their time outside of school. However, summer is not all fun and games. For children with learning needs, this is also a time of “
The end of the school year is almost near. Soon many of our clients with language and literacy difficulties will be going on summer vacation and enjoying their time outside of school. However, summer is not all fun and games. For children with learning needs, this is also a time of “ In the past, I have written several posts on the topic of word finding difficulties (
In the past, I have written several posts on the topic of word finding difficulties ( I enjoyed
I enjoyed 


 In my social pragmatic language groups I target a wide variety of social communication goals for children with varying levels and degrees of impairment with a focus on improving their social pragmatic language competence. In the past I have written blog posts on a variety of social pragmatic language therapy topics, including strategies for
In my social pragmatic language groups I target a wide variety of social communication goals for children with varying levels and degrees of impairment with a focus on improving their social pragmatic language competence. In the past I have written blog posts on a variety of social pragmatic language therapy topics, including strategies for 


 In the past, I have written about why
In the past, I have written about why