
Assessment of Social Communication Deficits in School-Aged Children


 Those of you familiar with my blog, know that a number of my posts take on a form of extended responses to posts and comments on social media which deal with certain questionable speech pathology trends and ongoing issues (e.g., controversial diagnostic labels, questionable recommendations, non-evidence based practices, etc.). So, today, I’d like to talk about sweeping general recommendations as pertaining to literacy interventions. Continue reading But is this the Best Practice Recommendation?
Those of you familiar with my blog, know that a number of my posts take on a form of extended responses to posts and comments on social media which deal with certain questionable speech pathology trends and ongoing issues (e.g., controversial diagnostic labels, questionable recommendations, non-evidence based practices, etc.). So, today, I’d like to talk about sweeping general recommendations as pertaining to literacy interventions. Continue reading But is this the Best Practice Recommendation?

 Recently I read a terrific article written in 2014 by Sun and Wallach entitled: “Language Disorders Are Learning Disabilities: Challenges on the Divergent and Diverse Paths to Language Learning Disability“. I found it to be so valuable that I wanted to summarize some of its key points to my readers because it bears tremendous impact on our understanding of what happens to children with language disorders when they reach school years.
Recently I read a terrific article written in 2014 by Sun and Wallach entitled: “Language Disorders Are Learning Disabilities: Challenges on the Divergent and Diverse Paths to Language Learning Disability“. I found it to be so valuable that I wanted to summarize some of its key points to my readers because it bears tremendous impact on our understanding of what happens to children with language disorders when they reach school years.
The authors begin the article by introducing a scenario familiar to numerous SLPs. A young child is diagnosed with receptive, expressive and social pragmatic language deficits as a toddler (2.5 years of age) begins to receive speech language services, which continue through preschool and elementary school until 2nd grade. The child is receiving therapy under the diagnosis of specific language impairment (SLI), which is characterized by difficulties with acquiring language in the absence of any other known disorders. By 2nd grade the child has seemingly “caught up” in the areas of listening comprehension and complex sentence production but is now struggling academically in the areas of reading and writing. Now his teachers are concerned that he has a learning disability, and his bewildered parent asks “Is it true that my child now has another problem on top of his language problem?”
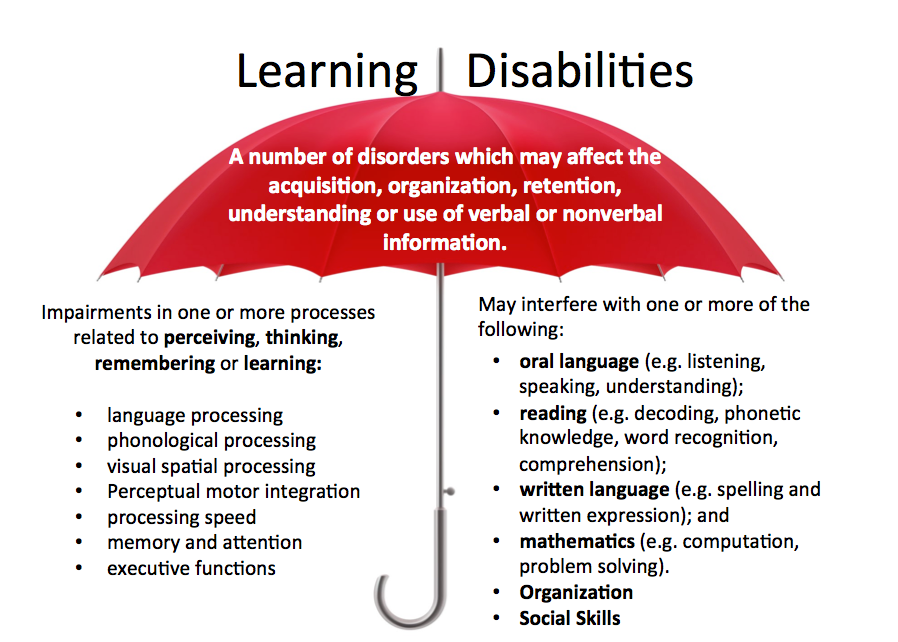
From that scenario the authors skillfully navigate the complex relationship between language disorders and school disability labels to explain that the child does NOT have a new disorder but rather continues to face new challenges presented by his old disorder due to which he is now struggling to meet the growing language demands of the academic curriculum.

Here’s the approximate hierarchy of language development in young children:
The problem is that if the child experiences any deficits in the foundational language areas such as listening and speaking, he will most certainly experience difficulties in the more complex areas of language which is reading and writing.
The authors continue by explaining the complexity of various labels given to children with language and learning difficulties under the IDEA 2004, DSM-5, as well as “research literature and nonschool clinical settings”. They conclude that: “the use of different labels by different professionals in different contexts should not obscure the commonalities among children with language disorders, no matter what they are called”.

Then they go on to explain that longitudinal (over a period of time) research has revealed numerous difficulties experienced by children with “early language disorders” during school years and in adulthood “in all domains of academic achievement (spelling, reading comprehension, word identification, word attack, calculation)…”. They also point out that many of these children with language disorders were later classified with a learning disability because their “later learning difficulties [took on] the form of problems acquiring higher levels of spoken language comprehension and expression as well as reading and writing”.
The authors also explain the complex process of literacy acquisition as well as discuss the important concept of “illusory recovery“. They note that there may be “a time period when the students with early language disorders seem to catch up with their typically developing peers” by undergoing a “spurt” in language learning, which is followed by a “postspurt plateau” because due to their ongoing deficits and an increase in academic demands “many children with early language disorders fail to “outgrow” these difficulties or catch up with their typically developing peers”.
They pointed out that because many of these children “may not show academic or language-related learning difficulties until linguistic and cognitive demands of the task increase and exceed their limited abilities”, SLPs must consider the “underlying deficits that may be masked by early oral language development” and “evaluate a child’s language abilities in all modalities, including preliteracy, literacy, and metalinguistic skills”.

Finally, the authors reiterate that since language is embedded in all parts of the curriculum “intervention choices should be based on students’ ongoing language learning and literacy problems within curricular contexts, regardless of their diagnostic labels”. In other words, SLPs should actively use the students’ curriculum in the intervention process.
In their conclusion the authors summarize the key article points:
I hope that you’ve found this article helpful in furthering your understanding of these highly relevant yet often misunderstood labels and that this knowledge will assist you to make better decisions when serving the clients on your caseload.
References:
Helpful Smart Speech Therapy Resources:
September is quickly approaching and school-based speech language pathologists (SLPs) are preparing to go back to work. Many of them are looking to update their arsenal of speech and language materials for the upcoming academic school year.
With that in mind, I wanted to update my readers regarding all the new products I have recently created with a focus on assessment and treatment in speech language pathology. Continue reading New Products for the 2017 Academic School Year for SLPs
 A few days ago I posted my first installment in the comprehensive assessment of dyslexia series, discussing common dyslexia myths as well as general language testing as a starting point in the dyslexia testing battery. (You can find this post HERE).
A few days ago I posted my first installment in the comprehensive assessment of dyslexia series, discussing common dyslexia myths as well as general language testing as a starting point in the dyslexia testing battery. (You can find this post HERE).
Today I would like to discuss the next two steps in dyslexia assessment, which are phonological awareness and word fluency testing.
Let’s begin with phonological awareness (PA). Phonological awareness is a precursor to emergent reading. It allows children to understand and manipulate sounds in order to form or breakdown words. It’s one of those interesting types of knowledge, which is a prerequisite to everything and is definitive of nothing. I like to compare it to taking a statistics course in college. You need it as a prerequisite to entering a graduate speech pathology program but just because you successfully complete it does not mean that you will graduate the program. Similarly, the children need to have phonological awareness mastery in order to move on and build upon existing skills to become emergent readers, however, simply having this mastery does not a good reader make (hence this is only one of the tests in dyslexia battery).
When a child has poor phonological awareness for his/her age it is a red flag for reading disabilities. Thus it is very important to assess the child’s ability to successfully manipulate sounds (e.g., by isolating, segmenting, blending, etc.,) in order to produce real or nonsense words.
Why are nonsense words important?
According to Shaywitz (2003), “The ability to read nonsense words is the best measure of phonological decoding skill in children.” (p. 133-134) Being able to decode and manipulate (blend, segment, etc.) nonsense words is a good indication that the child is acquiring comprehension of the alphabetic principle (understands sound letter correspondence or what common sounds are made by specific letters). It is a very important part of a dyslexia battery since nonsense words cannot be memorized or guessed but need to be “truly decoded.”
While a number of standardized tests assess phonological awareness skills, my personal preference is the Comprehensive Test of Phonological Processing-2 (CTOPP-2), which assesses the following areas:
As you can see from above description, it not only assesses the children’s ability to manipulate real words but also their ability to manipulate nonsense words. It also assesses word fluency skills via a host of rapid naming tasks, so it’s a very convenient tool to have as part of your dyslexia testing battery.
This brings us to another integral part of the dyslexia testing battery which is word fluency testing (WF). During word fluency tasks a child is asked to rapidly generate words on a particular topic given timed constraints (e.g., name as many animals as you can in 1 minute, etc.). We test this rapid naming ability because we want to see how quickly and accurately the child can process information. This ability is very much needed to become a fluent reader.
Poor readers can name a number of items but they may not be able to efficiently categorize these words. Furthermore, they will produce the items with a significantly decreased processing speed as compared to good readers. Decreased word fluency is a significant indicator of reading deficits. It is frequently observable in children with reading disabilities when they encounter a text with which they lack familiarity. That is why this ability is very important to test.
Several tests can be used for this purpose including CTOPP-2 and Rapid Automatized Naming and Rapid Alternating Stimulus Test (RAN/RAS) just to name a few. However, since CTOPP-2 already has a number of subtests which deal with testing this skill, I prefer to use it to test both phonological awareness and word fluency.
Read part III of this series which discusses components of Reading Fluency and Reading Comprehension testing HERE.
 As an SLP who routinely conducts speech and language assessments in several settings (e.g., school and private practice), I understand the utility of and the need for standardized speech, language, and literacy tests. However, as an SLP who works with children with dramatically varying degree of cognition, abilities, and skill-sets, I also highly value supplementing these standardized tests with functional and dynamic assessments, interactions, and observations.
As an SLP who routinely conducts speech and language assessments in several settings (e.g., school and private practice), I understand the utility of and the need for standardized speech, language, and literacy tests. However, as an SLP who works with children with dramatically varying degree of cognition, abilities, and skill-sets, I also highly value supplementing these standardized tests with functional and dynamic assessments, interactions, and observations.
 Since a significant value is placed on standardized testing by both schools and insurance companies for the purposes of service provision and reimbursement, I wanted to summarize in today’s post the findings of recent articles on this topic. Since my primary interest lies in assessing and treating school-age children, for the purposes of today’s post all of the reviewed articles came directly from the Language Speech and Hearing Services in Schools (LSHSS) journal.
Since a significant value is placed on standardized testing by both schools and insurance companies for the purposes of service provision and reimbursement, I wanted to summarize in today’s post the findings of recent articles on this topic. Since my primary interest lies in assessing and treating school-age children, for the purposes of today’s post all of the reviewed articles came directly from the Language Speech and Hearing Services in Schools (LSHSS) journal.
We’ve all been there. We’ve all had situations in which students scored on the low end of normal, or had a few subtest scores in the below average range, which equaled an average total score. We’ve all poured over eligibility requirements trying to figure out whether the student should receive therapy services given the stringent standardized testing criteria in some states/districts.
Of course, as it turns out, the answer is never simple. In 2006, Spaulding, Plante & Farinella set out to examine the assumption: “that children with language impairment will receive low scores on standardized tests, and therefore [those] low scores will accurately identify these children” (61). So they analyzed the data from 43 commercially available child language tests to identify whether evidence exists to support their use in identifying language impairment in children.
 Turns out it did not! Turns out due to the variation in psychometric properties of various tests (see article for specific details), many children with language impairment are overlooked by standardized tests by receiving scores within the average range or not receiving low enough scores to qualify for services. Thus, “the clinical consequence is that a child who truly has a language impairment has a roughly equal chance of being correctly or incorrectly identified, depending on the test that he or she is given.” Furthermore, “even if a child is diagnosed accurately as language impaired at one point in time, future diagnoses may lead to the false perception that the child has recovered, depending on the test(s) that he or she has been given (69).”
Turns out it did not! Turns out due to the variation in psychometric properties of various tests (see article for specific details), many children with language impairment are overlooked by standardized tests by receiving scores within the average range or not receiving low enough scores to qualify for services. Thus, “the clinical consequence is that a child who truly has a language impairment has a roughly equal chance of being correctly or incorrectly identified, depending on the test that he or she is given.” Furthermore, “even if a child is diagnosed accurately as language impaired at one point in time, future diagnoses may lead to the false perception that the child has recovered, depending on the test(s) that he or she has been given (69).”
Consequently, they created a decision tree (see below) with recommendations for clinicians using standardized testing. They recommend using alternate sources of data (sensitivity and specificity rates) to support accurate identification (available for a small subset of select tests).

The idea behind it is: “if sensitivity and specificity data are strong, and these data were derived from subjects who are comparable to the child tested, then the clinician can be relatively confident in relying on the test score data to aid his or her diagnostic decision. However, if the data are weak, then more caution is warranted and other sources of information on the child’s status might have primacy in making a diagnosis (70).”
Fast forward 6 years, and a number of newly revised tests later, in 2012, Spaulding and colleagues set out to “identify various U.S. state education departments’ criteria for determining the severity of language impairment in children, with particular focus on the use of norm-referenced tests” as well as to “determine if norm-referenced tests of child language were developed for the purpose of identifying the severity of children’s language impairment” (176).
They obtained published procedures for severity determinations from available U.S. state education departments, which specified the use of norm-referenced tests, and reviewed the manuals for 45 norm-referenced tests of child language to determine if each test was designed to identify the degree of a child’s language impairment.
What they found out was “the degree of use and cutoff-point criteria for severity determination varied across states. No cutoff-point criteria aligned with the severity cutoff points described within the test manuals. Furthermore, tests that included severity information lacked empirical data on how the severity categories were derived (176).”
 Thus they urged SLPs to exercise caution in determining the severity of children’s language impairment via norm-referenced test performance “given the inconsistency in guidelines and lack of empirical data within test manuals to support this use (176)”.
Thus they urged SLPs to exercise caution in determining the severity of children’s language impairment via norm-referenced test performance “given the inconsistency in guidelines and lack of empirical data within test manuals to support this use (176)”.
Following the publication of this article, Ireland, Hall-Mills & Millikin issued a response to the Spaulding and colleagues article. They pointed out that the “severity of language impairment is only one piece of information considered by a team for the determination of eligibility for special education and related services”. They noted that they left out a host of federal and state guideline requirements and “did not provide an analysis of the regulations governing special education evaluation and criteria for determining eligibility (320).” They pointed out that “IDEA prohibits the use of ‘any single measure or assessment as the sole criterion’ for determination of disability and requires that IEP teams ‘draw upon information from a variety of sources.”
They listed a variety of examples from several different state departments of education (FL, NC, VA, etc.), which mandate the use of functional assessments, dynamic assessments criterion-referenced assessments, etc. for their determination of language therapy eligibility.
 But are the SLPs from across the country appropriately using the federal and state guidelines in order to determine eligibility? While one should certainly hope so, it does not always seem to be the case. To illustrate, in 2012, Betz & colleagues asked 364 SLPs to complete a survey “regarding how frequently they used specific standardized tests when diagnosing suspected specific language impairment (SLI) (133).”
But are the SLPs from across the country appropriately using the federal and state guidelines in order to determine eligibility? While one should certainly hope so, it does not always seem to be the case. To illustrate, in 2012, Betz & colleagues asked 364 SLPs to complete a survey “regarding how frequently they used specific standardized tests when diagnosing suspected specific language impairment (SLI) (133).”
Their purpose was to determine “whether the quality of standardized tests, as measured by the test’s psychometric properties, is related to how frequently the tests are used in clinical practice” (133).
What they found out was that the most frequently used tests were the comprehensive assessments including the Clinical Evaluation of Language Fundamentals and the Preschool Language Scale as well as one word vocabulary tests such as the Peabody Picture Vocabulary Test. Furthermore, the date of publication seemed to be the only factor which affected the frequency of test selection.
They also found out that frequently SLPs did not follow up the comprehensive standardized testing with domain specific assessments (critical thinking, social communication, etc.) but instead used the vocabulary testing as a second measure. They were understandably puzzled by that finding. “The emphasis placed on vocabulary measures is intriguing because although vocabulary is often a weakness in children with SLI (e.g., Stothard et al., 1998), the research to date does not show vocabulary to be more impaired than other language domains in children with SLI (140).“
According to the authors, “perhaps the most discouraging finding of this study was the lack of a correlation between frequency of test use and test accuracy, measured both in terms of sensitivity/specificity and mean difference scores (141).”
If since the time (2012) SLPs have not significantly change their practices, the above is certainly disheartening, as it implies that rather than being true diagnosticians, SLPs are using whatever is at hand that has been purchased by their department to indiscriminately assess students with suspected speech language disorders. If that is truly the case, it certainly places into question the Ireland, Hall-Mills & Millikin’s response to Spaulding and colleagues. In other words, though SLPs are aware that they need to comply with state and federal regulations when it comes to unbiased and targeted assessments of children with suspected language disorders, they may not actually be using appropriate standardized testing much less supplementary informal assessments (e.g., dynamic, narrative, language sampling) in order to administer well-rounded assessments.
 So where do we go from here? Well, it’s quite simple really! We already know what the problem is. Based on the above articles we know that:
So where do we go from here? Well, it’s quite simple really! We already know what the problem is. Based on the above articles we know that:
Now that we have identified a problem, we need to develop and consistently implement effective practices to ameliorate it. These include researching psychometric properties of tests to review sample size, sensitivity and specificity, etc, use domain specific assessments to supplement administration of comprehensive testing, as well as supplement standardized testing with a plethora of functional assessments.
SLPs can review testing manuals and consult with colleagues when they feel that the standardized testing is underidentifying students with language impairments (e.g., HERE and HERE). They can utilize referral checklists (e.g., HERE) in order to pinpoint the students’ most significant difficulties. Finally, they can develop and consistently implement informal assessment practices (e.g., HERE and HERE) during testing in order to gain a better grasp on their students’ TRUE linguistic functioning.
Stay tuned for the second portion of this post entitled: “What Research Shows About the Functional Relevance of Standardized Speech Tests?” to find out the best practices in the assessment of speech sound disorders in children.
References:

Please note that this post was originally published in the Summer 2016 NJSHA’s VOICES (available HERE).
If you have been keeping up with new developments in the field of bilingualism then you’ve probably heard the term “translanguaging,” increasingly mentioned at bilingual conferences across the nation. If you haven’t, ‘translanguaging’ is the “ability of multilingual speakers to shuttle between languages, treating the diverse languages that form their repertoire as an integrated system” (Canagarajah, 2011, p. 401). In other words, translanguaging allows bilinguals to make “flexible use their linguistic resources to make meaning of their lives and their complex worlds” (Garcia, 2011, pg. 1).
 Wait a second, you might say! “Isn’t that a definition of ‘code-switching’?” And the answer is: “No!” The concept of ‘code-switching’ implies that bilinguals use two separate linguistic codes which do not overlap/reference each other. In contrast, ‘translanguaging’ assumes from the get-go that “bilinguals have one linguistic repertoire from which they select features strategically to communicate effectively” (Garcia, 2012, pg. 1). Bilinguals engage in translanguaging on an ongoing basis in their daily lives. They speak different languages to different individuals, find ‘Google’ translations of words and compare results from various online sites, listen to music in one language but watch TV in another, as well as watch TV announcers fluidly integrate several languages in their event narratives during news or in infomercials (Celic & Seltzer, 2011). For functional bilinguals, these practices are such integral part of their daily lives that they rarely realize just how much ‘translanguaging’ they actually do every day.
Wait a second, you might say! “Isn’t that a definition of ‘code-switching’?” And the answer is: “No!” The concept of ‘code-switching’ implies that bilinguals use two separate linguistic codes which do not overlap/reference each other. In contrast, ‘translanguaging’ assumes from the get-go that “bilinguals have one linguistic repertoire from which they select features strategically to communicate effectively” (Garcia, 2012, pg. 1). Bilinguals engage in translanguaging on an ongoing basis in their daily lives. They speak different languages to different individuals, find ‘Google’ translations of words and compare results from various online sites, listen to music in one language but watch TV in another, as well as watch TV announcers fluidly integrate several languages in their event narratives during news or in infomercials (Celic & Seltzer, 2011). For functional bilinguals, these practices are such integral part of their daily lives that they rarely realize just how much ‘translanguaging’ they actually do every day.
 One of the most useful features of translanguaging (and there are many) is that it assists with further development of bilinguals’ metalinguistic awareness abilities by allowing them to compare language practices as well as explicitly notice language features. Consequently, not only do speech-language pathologists (SLPs) need to be aware of translanguaging when working with culturally diverse clients, they can actually assist their clients make greater linguistic gains by embracing translanguaging practices. Furthermore, one does not have to be a bilingual SLP to incorporate translanguaging practices in the therapy room. Monolingual SLPs can certainly do it as well, and with a great degree of success.
One of the most useful features of translanguaging (and there are many) is that it assists with further development of bilinguals’ metalinguistic awareness abilities by allowing them to compare language practices as well as explicitly notice language features. Consequently, not only do speech-language pathologists (SLPs) need to be aware of translanguaging when working with culturally diverse clients, they can actually assist their clients make greater linguistic gains by embracing translanguaging practices. Furthermore, one does not have to be a bilingual SLP to incorporate translanguaging practices in the therapy room. Monolingual SLPs can certainly do it as well, and with a great degree of success.
 Here are some strategies of how this can be accomplished. Let us begin with bilingual SLPs who have the ability to do therapy in both languages. One great way to incorporate translanguaging in therapy is to alternate between English and the desired language (e.g., Spanish) throughout the session. Translanguaging strategies may include: using key vocabulary, grammar and syntax structures in both languages (side to side), alternating between English and Spanish websites when researching specific information (e.g., an animal habitats, etc.), asking students to take notes in both languages or combining two languages in one piece of writing. For younger preschool students, reading the same book, translated in another language is also a viable option as it increases their lexicon in both languages.
Here are some strategies of how this can be accomplished. Let us begin with bilingual SLPs who have the ability to do therapy in both languages. One great way to incorporate translanguaging in therapy is to alternate between English and the desired language (e.g., Spanish) throughout the session. Translanguaging strategies may include: using key vocabulary, grammar and syntax structures in both languages (side to side), alternating between English and Spanish websites when researching specific information (e.g., an animal habitats, etc.), asking students to take notes in both languages or combining two languages in one piece of writing. For younger preschool students, reading the same book, translated in another language is also a viable option as it increases their lexicon in both languages.
 Those SLPs who treat ESL students with language disorders and collaborate with ESL teachers can design thematic intervention with a focus on particular topics of interest. For example, during the month of April there’s increased attention on the topic of ‘human impact on the environment.’ Students can read texts on this topic in English and then use the internet to look up websites containing the information in their birth language. They can also listen to a translation or a summary of the English book in their birth language. Finally, they can make comparisons of human impact on the environment between United States and their birth/heritage countries.
Those SLPs who treat ESL students with language disorders and collaborate with ESL teachers can design thematic intervention with a focus on particular topics of interest. For example, during the month of April there’s increased attention on the topic of ‘human impact on the environment.’ Students can read texts on this topic in English and then use the internet to look up websites containing the information in their birth language. They can also listen to a translation or a summary of the English book in their birth language. Finally, they can make comparisons of human impact on the environment between United States and their birth/heritage countries.
As we are treating culturally and linguistically diverse students it is important to use self-questions such as: “Can we connect a particular content-area topic to our students’ cultures?” or “Can we include different texts or resources in sessions which represent our students’ multicultural perspectives?” which can assist us in making best decisions in their care (Celic & Seltzer, 2011).
 We can “Get to know our students” by displaying a world map in our therapy room/classroom and asking them to show us where they were born or came from (or where their family is from). We can label the map with our students’ names and photographs and provide them with the opportunity to discuss their culture and develop cultural connections. We can create a multilingual therapy room by using multilingual labels and word walls as well as sprinkling our English language therapy with words relevant to the students from their birth/heritage languages (e.g., songs and greetings, etc.).
We can “Get to know our students” by displaying a world map in our therapy room/classroom and asking them to show us where they were born or came from (or where their family is from). We can label the map with our students’ names and photographs and provide them with the opportunity to discuss their culture and develop cultural connections. We can create a multilingual therapy room by using multilingual labels and word walls as well as sprinkling our English language therapy with words relevant to the students from their birth/heritage languages (e.g., songs and greetings, etc.).

Monolingual SLPs who do not speak the child’s language or speak it very limitedly, can use multilingual books which contain words from other languages. To introduce just a few words in Spanish, books such as ‘Maňana Iguana’ by Ann Whitford Paul, ‘Count on Culebra’ by Ann Whitford Paul, ‘Abuela’ by Arthur Doros, or ‘Old man and his door’ by Gary Soto can be used. SLPs with greater proficiency in a particular language (e.g., Russian) they consider using dual bilingual books in sessions (e.g., ‘Goldilocks and the Three Bears’ by Kate Clynes, ‘Giant Turnip’ by Henriette Barkow. All of these books can be found on such websites as ‘Amazon’ (string search: children’s foreign language books), ‘Language Lizard’ or ‘Trilingual Mama’ (contains list of free online multilingual books).
It is also important to understand that many of our language impaired bilingual students have a very limited knowledge of the world beyond the “here and now.” Many upper elementary and middle school youngsters have difficulty naming world’s continents, and do not know the names and capitals of major countries. That is why it is also important to teach them general concepts of geography, discuss world’s counties and the people who live there, as well as introduce them to select multicultural holidays celebrated in United States and in other countries around the world.
All students benefit from translanguaging! It increases awareness of language diversity in monolingual students, validates use of home languages for bilingual students, as well as assists with teaching challenging academic content and development of English for emergent bilingual students. Translanguaging can take place in any classroom or therapy room with any group of children including those with primary language impairments or those speaking different languages from one another. The cognitive benefits of translanguaging are numerous because it allows students to use all of their languages as a resource for learning, reading, writing, and thinking in the classroom (Celic & Seltzer, 2011).
References:
Helpful Smart Speech Therapy Resources: