 Several years ago I wrote a post about how to perform clinical reading assessments of adolescent students. Today I am writing a follow-up post with a focus on the clinical reading assessment of elementary-aged students. For this purpose, I often use the books from the Continental Press series entitled: Content Reading for Geography, Social Studies, & Science. Texts for grades 2-7 of the series are perfect for assessment of struggling elementary-aged readers. Continue reading Clinical Assessment of Reading Abilities of Elementary Aged Children
Several years ago I wrote a post about how to perform clinical reading assessments of adolescent students. Today I am writing a follow-up post with a focus on the clinical reading assessment of elementary-aged students. For this purpose, I often use the books from the Continental Press series entitled: Content Reading for Geography, Social Studies, & Science. Texts for grades 2-7 of the series are perfect for assessment of struggling elementary-aged readers. Continue reading Clinical Assessment of Reading Abilities of Elementary Aged Children
Search Results for: dyslexia%20testing
What Makes an Independent Speech-Language-Literacy Evaluation a GOOD Evaluation?
 Three years ago I wrote a blog post entitled: “Special Education Disputes and Comprehensive Language Testing: What Parents, Attorneys, and Advocates Need to Know“. In it, I used 4 very different scenarios to illustrate the importance of comprehensive language evaluations for children with subtle language and learning needs. Today I would like to expound more on that post in order to explain, what actually constitutes a good independent comprehensive assessment. Continue reading What Makes an Independent Speech-Language-Literacy Evaluation a GOOD Evaluation?
Three years ago I wrote a blog post entitled: “Special Education Disputes and Comprehensive Language Testing: What Parents, Attorneys, and Advocates Need to Know“. In it, I used 4 very different scenarios to illustrate the importance of comprehensive language evaluations for children with subtle language and learning needs. Today I would like to expound more on that post in order to explain, what actually constitutes a good independent comprehensive assessment. Continue reading What Makes an Independent Speech-Language-Literacy Evaluation a GOOD Evaluation?
Treatment of Children with “APD”: What SLPs Need to Know
 In recent years there has been an increase in research on the subject of diagnosis and treatment of Auditory Processing Disorders (APD), formerly known as Central Auditory Processing Disorders or CAPD.
In recent years there has been an increase in research on the subject of diagnosis and treatment of Auditory Processing Disorders (APD), formerly known as Central Auditory Processing Disorders or CAPD.
More and more studies in the fields of audiology and speech-language pathology began confirming the lack of validity of APD as a standalone (or useful) diagnosis. To illustrate, in June 2015, the American Journal of Audiology published an article by David DeBonis entitled: “It Is Time to Rethink Central Auditory Processing Disorder Protocols for School-Aged Children.” In this article, DeBonis pointed out numerous inconsistencies involved in APD testing and concluded that “routine use of APD test protocols cannot be supported” and that [APD] “intervention needs to be contextualized and functional” (DeBonis, 2015, p. 124) Continue reading Treatment of Children with “APD”: What SLPs Need to Know
Making Our Interventions Count or What’s Research Got To Do With It?
 Two years ago I wrote a blog post entitled: “What’s Memes Got To Do With It?” which summarized key points of Dr. Alan G. Kamhi’s 2004 article: “A Meme’s Eye View of Speech-Language Pathology“. It delved into answering the following question: “Why do some terms, labels, ideas, and constructs [in our field] prevail whereas others fail to gain acceptance?”.
Two years ago I wrote a blog post entitled: “What’s Memes Got To Do With It?” which summarized key points of Dr. Alan G. Kamhi’s 2004 article: “A Meme’s Eye View of Speech-Language Pathology“. It delved into answering the following question: “Why do some terms, labels, ideas, and constructs [in our field] prevail whereas others fail to gain acceptance?”.
Today I would like to reference another article by Dr. Kamhi written in 2014, entitled “Improving Clinical Practices for Children With Language and Learning Disorders“.
This article was written to address the gaps between research and clinical practice with respect to the implementation of EBP for intervention purposes.
Dr. Kamhi begins the article by posing 10 True or False questions for his readers:
- Learning is easier than generalization.
- Instruction that is constant and predictable is more effective than instruction that varies the conditions of learning and practice.
- Focused stimulation (massed practice) is a more effective teaching strategy than varied stimulation (distributed practice).
- The more feedback, the better.
- Repeated reading of passages is the best way to learn text information.
- More therapy is always better.
- The most effective language and literacy interventions target processing limitations rather than knowledge deficits.
- Telegraphic utterances (e.g., push ball, mommy sock) should not be provided as input for children with limited language.
- Appropriate language goals include increasing levels of mean length of utterance (MLU) and targeting Brown’s (1973) 14 grammatical morphemes.
- Sequencing is an important skill for narrative competence.
Guess what? Only statement 8 of the above quiz is True! Every other statement from the above is FALSE!
Now, let’s talk about why that is!
 First up is the concept of learning vs. generalization. Here Dr. Kamhi discusses that some clinicians still possess an “outdated behavioral view of learning” in our field, which is not theoretically and clinically useful. He explains that when we are talking about generalization – what children truly have a difficulty with is “transferring narrow limited rules to new situations“. “Children with language and learning problems will have difficulty acquiring broad-based rules and modifying these rules once acquired, and they also will be more vulnerable to performance demands on speech production and comprehension (Kamhi, 1988)” (93). After all, it is not “reasonable to expect children to use language targets consistently after a brief period of intervention” and while we hope that “language intervention [is] designed to lead children with language disorders to acquire broad-based language rules” it is a hugely difficult task to undertake and execute.
First up is the concept of learning vs. generalization. Here Dr. Kamhi discusses that some clinicians still possess an “outdated behavioral view of learning” in our field, which is not theoretically and clinically useful. He explains that when we are talking about generalization – what children truly have a difficulty with is “transferring narrow limited rules to new situations“. “Children with language and learning problems will have difficulty acquiring broad-based rules and modifying these rules once acquired, and they also will be more vulnerable to performance demands on speech production and comprehension (Kamhi, 1988)” (93). After all, it is not “reasonable to expect children to use language targets consistently after a brief period of intervention” and while we hope that “language intervention [is] designed to lead children with language disorders to acquire broad-based language rules” it is a hugely difficult task to undertake and execute.
Next, Dr. Kamhi addresses the issue of instructional factors, specifically the importance of “varying conditions of instruction and practice“. Here, he addresses the fact that while contextualized instruction is highly beneficial to learners unless we inject variability and modify various aspects of instruction including context, composition, duration, etc., we ran the risk of limiting our students’ long-term outcomes.
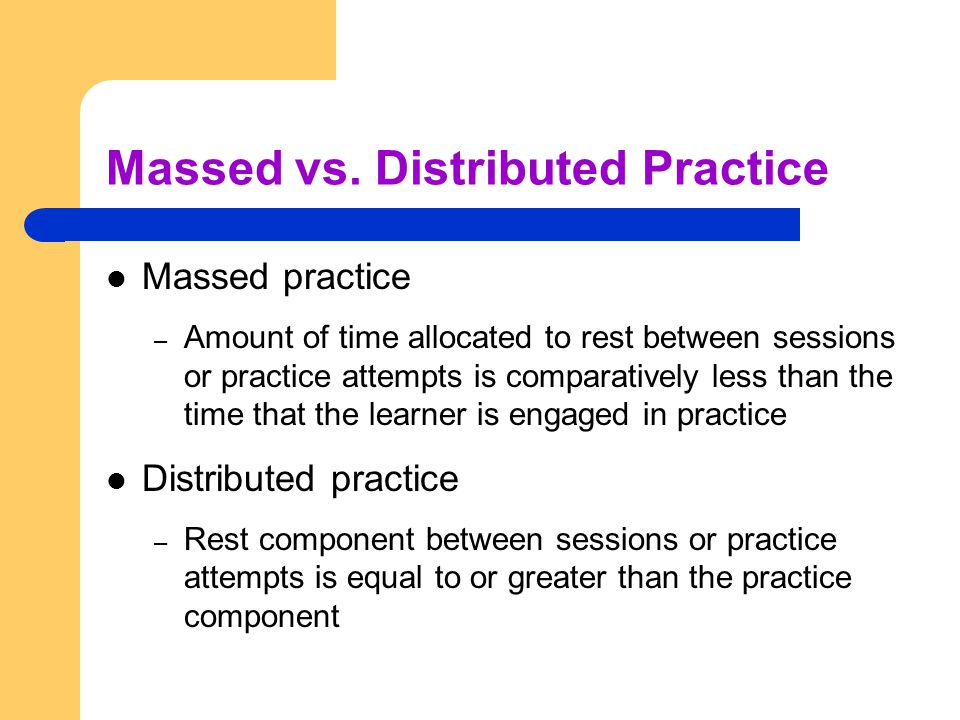 After that, Dr. Kamhi addresses the concept of distributed practice (spacing of intervention) and how important it is for teaching children with language disorders. He points out that a number of recent studies have found that “spacing and distribution of teaching episodes have more of an impact on treatment outcomes than treatment intensity” (94).
After that, Dr. Kamhi addresses the concept of distributed practice (spacing of intervention) and how important it is for teaching children with language disorders. He points out that a number of recent studies have found that “spacing and distribution of teaching episodes have more of an impact on treatment outcomes than treatment intensity” (94).
He also advocates reducing evaluative feedback to learners to “enhance long-term retention and generalization of motor skills“. While he cites research from studies pertaining to speech production, he adds that language learning could also benefit from this practice as it would reduce conversational disruptions and tunning out on the part of the student.
From there he addresses the limitations of repetition for specific tasks (e.g., text rereading). He emphasizes how important it is for students to recall and retrieve text rather than repeatedly reread it (even without correction), as the latter results in a lack of comprehension/retention of read information.
After that, he discusses treatment intensity. Here he emphasizes the fact that higher dose of instruction will not necessarily result in better therapy outcomes due to the research on the effects of “learning plateaus and threshold effects in language and literacy” (95). We have seen research on this with respect to joint book reading, vocabulary words exposure, etc. As such, at a certain point in time increased intensity may actually result in decreased treatment benefits.
 His next point against processing interventions is very near and dear to my heart. Those of you familiar with my blog know that I have devoted a substantial number of posts pertaining to the lack of validity of CAPD diagnosis (as a standalone entity) and urged clinicians to provide language based vs. specific auditory interventions which lack treatment utility. Here, Dr. Kamhi makes a great point that: “Interventions that target processing skills are particularly appealing because they offer the promise of improving language and learning deficits without having to directly target the specific knowledge and skills required to be a proficient speaker, listener, reader, and writer.” (95) The problem is that we have numerous studies on the topic of improvement of isolated skills (e.g., auditory skills, working memory, slow processing, etc.) which clearly indicate lack of effectiveness of these interventions. As such, “practitioners should be highly skeptical of interventions that promise quick fixes for language and learning disabilities” (96).
His next point against processing interventions is very near and dear to my heart. Those of you familiar with my blog know that I have devoted a substantial number of posts pertaining to the lack of validity of CAPD diagnosis (as a standalone entity) and urged clinicians to provide language based vs. specific auditory interventions which lack treatment utility. Here, Dr. Kamhi makes a great point that: “Interventions that target processing skills are particularly appealing because they offer the promise of improving language and learning deficits without having to directly target the specific knowledge and skills required to be a proficient speaker, listener, reader, and writer.” (95) The problem is that we have numerous studies on the topic of improvement of isolated skills (e.g., auditory skills, working memory, slow processing, etc.) which clearly indicate lack of effectiveness of these interventions. As such, “practitioners should be highly skeptical of interventions that promise quick fixes for language and learning disabilities” (96).
Now let us move on to language and particularly the models we provide to our clients to encourage greater verbal output. Research indicates that when clinicians are attempting to expand children’s utterances, they need to provide well-formed language models. Studies show that children select strong input when its surrounded by weaker input (the surrounding weaker syllables make stronger syllables stand out). As such, clinicians should expand upon/comment on what clients are saying with grammatically complete models vs. telegraphic productions.
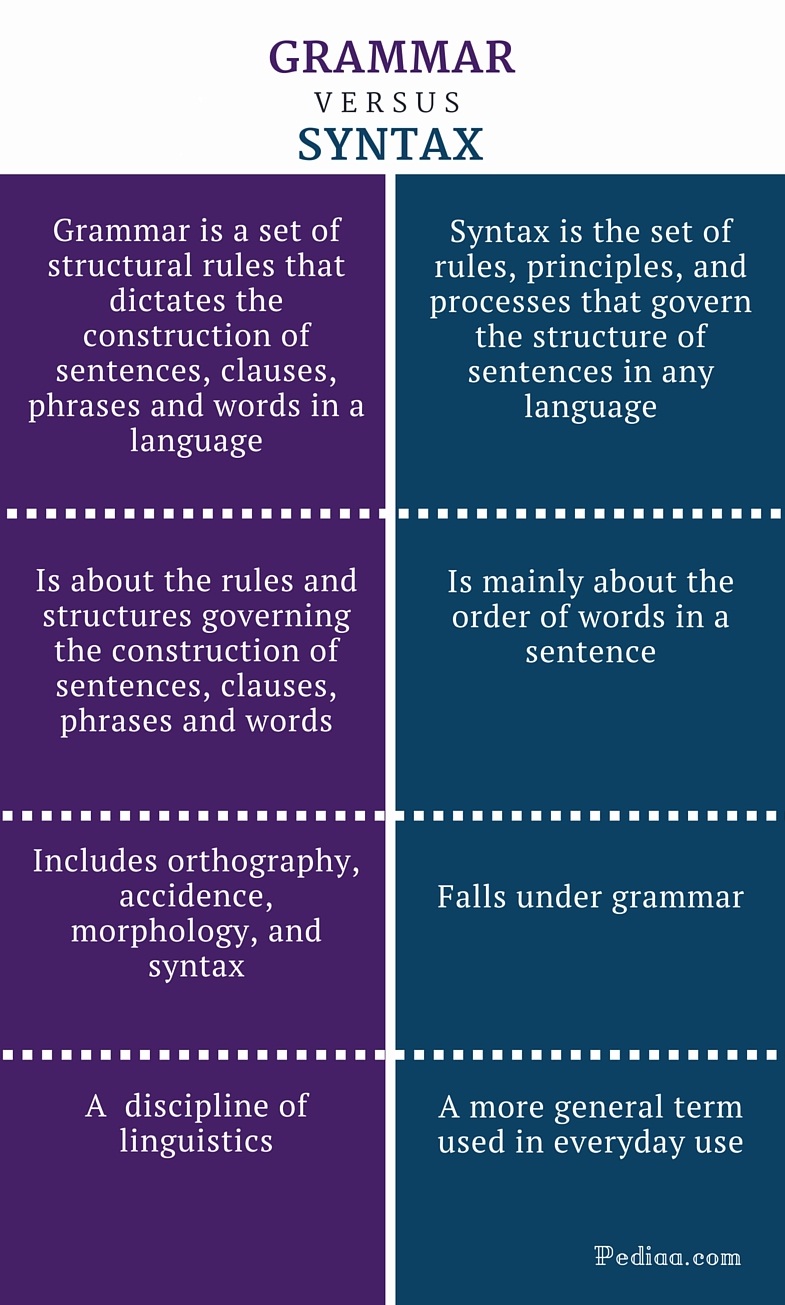 From there lets us take a look at Dr. Kamhi’s recommendations for grammar and syntax. Grammatical development goes much further than addressing Brown’s morphemes in therapy and calling it a day. As such, it is important to understand that children with developmental language disorders (DLD) (#DevLang) do not have difficulty acquiring all morphemes. Rather studies have shown that they have difficulty learning grammatical morphemes that reflect tense and agreement (e.g., third-person singular, past tense, auxiliaries, copulas, etc.). As such, use of measures developed by Hadley & Holt, 2006; Hadley & Short, 2005 (e.g., Tense Marker Total & Productivity Score) can yield helpful information regarding which grammatical structures to target in therapy.
From there lets us take a look at Dr. Kamhi’s recommendations for grammar and syntax. Grammatical development goes much further than addressing Brown’s morphemes in therapy and calling it a day. As such, it is important to understand that children with developmental language disorders (DLD) (#DevLang) do not have difficulty acquiring all morphemes. Rather studies have shown that they have difficulty learning grammatical morphemes that reflect tense and agreement (e.g., third-person singular, past tense, auxiliaries, copulas, etc.). As such, use of measures developed by Hadley & Holt, 2006; Hadley & Short, 2005 (e.g., Tense Marker Total & Productivity Score) can yield helpful information regarding which grammatical structures to target in therapy.
With respect to syntax, Dr. Kamhi notes that many clinicians erroneously believe that complex syntax should be targeted when children are much older. The Common Core State Standards do not help this cause further, since according to the CCSS complex syntax should be targeted 2-3 grades, which is far too late. Typically developing children begin developing complex syntax around 2 years of age and begin readily producing it around 3 years of age. As such, clinicians should begin targeting complex syntax in preschool years and not wait until the children have mastered all morphemes and clauses (97)
Finally, Dr. Kamhi wraps up his article by offering suggestions regarding prioritizing intervention goals. Here, he explains that goal prioritization is affected by
- clinician experience and competencies
- the degree of collaboration with other professionals
- type of service delivery model
- client/student factors
He provides a hypothetical case scenario in which the teaching responsibilities are divvied up between three professionals, with SLP in charge of targeting narrative discourse. Here, he explains that targeting narratives does not involve targeting sequencing abilities. “The ability to understand and recall events in a story or script depends on conceptual understanding of the topic and attentional/memory abilities, not sequencing ability.” He emphasizes that sequencing is not a distinct cognitive process that requires isolated treatment. Yet many SLPs “continue to believe that sequencing is a distinct processing skill that needs to be assessed and treated.” (99)
 Dr. Kamhi supports the above point by providing an example of two passages. One, which describes a random order of events, and another which follows a logical order of events. He then points out that the randomly ordered story relies exclusively on attention and memory in terms of “sequencing”, while the second story reduces demands on memory due to its logical flow of events. As such, he points out that retelling deficits seemingly related to sequencing, tend to be actually due to “limitations in attention, working memory, and/or conceptual knowledge“. Hence, instead of targeting sequencing abilities in therapy, SLPs should instead use contextualized language intervention to target aspects of narrative development (macro and microstructural elements).
Dr. Kamhi supports the above point by providing an example of two passages. One, which describes a random order of events, and another which follows a logical order of events. He then points out that the randomly ordered story relies exclusively on attention and memory in terms of “sequencing”, while the second story reduces demands on memory due to its logical flow of events. As such, he points out that retelling deficits seemingly related to sequencing, tend to be actually due to “limitations in attention, working memory, and/or conceptual knowledge“. Hence, instead of targeting sequencing abilities in therapy, SLPs should instead use contextualized language intervention to target aspects of narrative development (macro and microstructural elements).
Furthermore, here it is also important to note that the “sequencing fallacy” affects more than just narratives. It is very prevalent in the intervention process in the form of the ubiquitous “following directions” goal/s. Many clinicians readily create this goal for their clients due to their belief that it will result in functional therapeutic language gains. However, when one really begins to deconstruct this goal, one will realize that it involves a number of discrete abilities including: memory, attention, concept knowledge, inferencing, etc. Consequently, targeting the above goal will not result in any functional gains for the students (their memory abilities will not magically improve as a result of it). Instead, targeting specific language and conceptual goals (e.g., answering questions, producing complex sentences, etc.) and increasing the students’ overall listening comprehension and verbal expression will result in improvements in the areas of attention, memory, and processing, including their ability to follow complex directions.
 There you have it! Ten practical suggestions from Dr. Kamhi ready for immediate implementation! And for more information, I highly recommend reading the other articles in the same clinical forum, all of which possess highly practical and relevant ideas for therapeutic implementation. They include:
There you have it! Ten practical suggestions from Dr. Kamhi ready for immediate implementation! And for more information, I highly recommend reading the other articles in the same clinical forum, all of which possess highly practical and relevant ideas for therapeutic implementation. They include:
- Clinical Scientists Improving Clinical Practices: In Thoughts and Actions
- Approaching Early Grammatical Intervention From a Sentence-Focused Framework
- What Works in Therapy: Further Thoughts on Improving Clinical Practice for Children With Language Disorders
- Improving Clinical Practice: A School-Age and School-Based Perspective
- Improving Clinical Services: Be Aware of Fuzzy Connections Between Principles and Strategies
- One Size Does Not Fit All: Improving Clinical Practice in Older Children and Adolescents With Language and Learning Disorders
- Language Intervention at the Middle School: Complex Talk Reflects Complex Thought
- Using Our Knowledge of Typical Language Development
References:
Kamhi, A. (2014). Improving clinical practices for children with language and learning disorders. Language, Speech, and Hearing Services in Schools, 45(2), 92-103
Helpful Social Media Resources:
Review and Giveaway of Strategies by Numbers (by SPELL-Links)
Today I am reviewing a fairly recently released (2014) book from the Learning By Design, Inc. team entitled SPELL-Links Strategies by Numbers. This 57 page instructional guide was created to support the implementation of the SPELL-Links to Reading and Writing Word Study Curriculum as well as to help students “use the SPELL-Links strategies anytime in any setting.’ (p. iii) Its purpose is to enable students to strategize their way to writing and reading rather than overrelying on memorization techniques.
SPELL-Links Strategies by Numbers contains in-depth explanations of SPELL-Links’ 14 strategies for spelling and reading, detailed instructions on how to teach the strategies during writing and reading activities, as well as helpful ideas for supporting students as they further acquire literacy skills. It can be used by a wide array of professionals including classroom teachers, speech-language pathologists, reading improvement teachers, learning disabilities teachers, aides, tutors, as well as parents for teaching word study lessons or as carryover and practice during reading and writing tasks.
The author includes a list of key terms used in the book as well as a guide with instructional icons 

The goal of the 14 strategies listed in the book is to build vocabulary, improve spelling, word decoding, reading fluency, and reading comprehension as well as improve students’ writing skills. While each strategy is presented in isolation under its own section, the end result is for students to fully integrate and apply multiple strategies when reading or writing.
Here’s the list of the 14 strategies in order of appearance as applied to spelling and reading:
- Sound It Out
- Check the Order
- Catch the Beat
- Listen Up
- A Little Stress Will Help This Mess
- No Fouls
- Play By the Rules
- Use Rhyme This Time
- Spell What You Mean and Mean What You Spell
- Be Smart About Word Parts
- Build on the Base
- Invite the Relatives
- Fix the Funny Stuff
- Look It Up
Each strategy includes highly detailed implementation instructions with students including pictorial support as well as both instructor and student guidance for practice at various levels during writing and reading tasks. At the end of the book all the strategies are succinctly summarized in handy table, which is also provided to the user separately as a double sided one page insert printed on reinforced paper to be used as a guide when the book is not handy.
There are a number of things I like about the book. Firstly, of course it is based on the latest research in reading, writing, and spelling. Secondly, clinicians can use it the absence of SPELL-Links to Reading and Writing Word Study Curriculum since the author’s purpose was to have the students “use the SPELL-Links strategies anytime in any setting.’ (p. iii). Thirdly, I love the fact that the book is based on the connectionist research model, which views spelling and reading as a “dynamic interplay of phonological, orthographic, and semantic knowledge.” (iii). Consequently, the listed strategies focus on simultaneously developing and strengthening phonological, orthographic, semantic and morphological knowledge during reading and writing tasks.
You can find this book for purchase on the Learning By Design, Inc. Store HERE. Finally, due to the generosity of Jan Wasowicz PhD the book’s author, you can enter my Rafflecopter giveaway below for a chance to win your own copy!
What do Auditory Memory Deficits Indicate in the Presence of Average General Language Scores?
 I frequently see a variation of the following question on a variety of speech language forums: “My student scored within the average range on all the tested subtests with the exception of working memory and sentence recall. What other testing do you recommend to determine whether these difficulties are impacting their academics?”
I frequently see a variation of the following question on a variety of speech language forums: “My student scored within the average range on all the tested subtests with the exception of working memory and sentence recall. What other testing do you recommend to determine whether these difficulties are impacting their academics?”
First, lets provide a definition of working memory (WM). WM is the memory used for temporarily storing and manipulating information so we can perform a particular task. It’s one of the executive functions (EFs) and contains two important subcomponents: a phonological loop that stores verbal information and a visuo-spatial ‘sketchpad’ which stores visual and spatial information (Baddeley & Hitch, 2007). Together they are responsible for acquisition of sound-letter correspondence, phonemic awareness and ultimately reading comprehension since WM influences the duration the information stays in memory as well as its eventual transfer (or lack of thereof) to long-term memory.
In other words, students with adequate working memory will have enough capacity to appropriately decode, fluently read and adequately comprehend text while students with poor working memory will expend all their capacity on basic tasks such as decoding, which leaves them with very little capacity to devote to comprehension of read material.
Outside of testing, WM deficits typically become glaringly apparent as students move up grade levels and are given challenging subject-specific abstract texts, requiring in-depth analysis. This is when parents and professionals start to see that in addition to experiencing difficulty comprehending the read texts, students with poor WM also tire easily when presented with lengthy texts, and tend to evidence increased frustration and decreased self-efficacy during reading tasks.
Now let’s get back to our original question: “What other testing do you recommend to determine whether these [memory] difficulties are impacting their academics?”
 Typically when asked that question I always tend to recommend that a trained SLP performs a series of tests aimed to determine whether the student presents with reading and writing deficits.
Typically when asked that question I always tend to recommend that a trained SLP performs a series of tests aimed to determine whether the student presents with reading and writing deficits.
In my clinical experience (which is of course substantiated by research) in 99% of cases, reading disabilities are the hidden culprit behind seemingly average oral language skills and working memory deficits. For more information on what testing is recommended to tease out the presence of reading disorders, see my series posts on Comprehensive Dyslexia Testing (HERE) as well as on the validity of (C)APD diagnosis (HERE).

So the next time you encounter this perplexing pattern of strengths and weaknesses don’t just ignore it as inconsequential and not recommend or dismiss the student from language services. Delve into it further! You will often find that it is representative of reading difficulties, the cumulative impact of which may significantly affect the student’s academic performance and ultimately school outcomes, unless appropriate therapeutic interventions are provided.
References:
- Baddeley, A. D., & Hitch, G. J. (2007). Working memory: Past, present…and future? In N.Osaka, R. Logie & M. D’Esposito (Eds), Working Memory – Behavioural & Neural Correlates. Oxford University Press.
Useful Resources:
Comprehensive Assessment of Adolescents with Suspected Language and Literacy Disorders
 When many of us think of such labels as “language disorder” or “learning disability”, very infrequently do adolescents (students 13-18 years of age) come to mind. Even today, much of the research in the field of pediatric speech pathology involves preschool and school-aged children under 12 years of age.
When many of us think of such labels as “language disorder” or “learning disability”, very infrequently do adolescents (students 13-18 years of age) come to mind. Even today, much of the research in the field of pediatric speech pathology involves preschool and school-aged children under 12 years of age.
The prevalence and incidence of language disorders in adolescents is very difficult to estimate due to which some authors even referred to them as a Neglected Group with Significant Problems having an “invisible disability“.
Far fewer speech language therapists work with middle-schoolers vs. preschoolers and elementary aged kids, while the numbers of SLPs working with high-school aged students is frequently in single digits in some districts while being completely absent in others. In fact, I am frequently told (and often see it firsthand) that some administrators try to cut costs by attempting to dictate a discontinuation of speech-language services on the grounds that adolescents “are far too old for services” or can “no longer benefit from services”.
But of course the above is blatantly false. Undetected language deficits don’t resolve with age! They simply exacerbate and turn into learning disabilities. Similarly, lack of necessary and appropriate service provision to children with diagnosed language impairments at the middle-school and high-school levels will strongly affect their academic functioning and hinder their future vocational outcomes.
A cursory look at the Speech Pathology Related Facebook Groups as well as ASHA forums reveals numerous SLPs in a continual search for best methods of assessment and treatment of older students (~12-18 years of age).
Consequently, today I wanted to dedicate this post to a review of standardized assessments options available for students 12-18 years of age with suspected language and literacy deficits.
Most comprehensive standardized assessments, “typically focus on semantics, syntax, morphology, and phonology, as these are the performance areas in which specific skill development can be most objectively measured” (Hill & Coufal, 2005, p 35). Very few of them actually incorporate aspects of literacy into its subtests in a meaningful way. Yet by the time students reach adolescence literacy begins to play an incredibly critical role not just in all the aspects of academics but also social communication.
So when it comes to comprehensive general language testing I highly recommended that SLPs select standardized measures with a focus on not language but also literacy. Presently of all the comprehensive assessment tools I highly prefer the Test of Integrated Language and Literacy (TILLS) for students up to 18 years of age, (see a comprehensive review HERE), which covers such literacy areas as phonological awareness, reading fluency, reading comprehension, writing and spelling in addition to traditional language areas as as vocabulary awareness, following directions, story recall, etc. However, while comprehensive tests have numerous uses, their sole administration will not constitute an adequate assessment.
So what areas should be assessed during language and literacy testing? Below are a few suggestions of standardized testing measures (and informal procedures) aimed at exploring the student abilities in particular areas pertaining to language and literacy.
TESTS OF LANGUAGE
- Listening Comprehension (for stories not just sentences)
- The Listening Comprehension Test-Adolescent (up to 18 years of age)
- Can be supplemented with informal listening comprehension assessment by giving the students grade level passages
- The Listening Comprehension Test-Adolescent (up to 18 years of age)
- Comprehension of Ambiguous and Figurative Language (e.g., idioms, ambiguous expressions, etc.)
- Clinical Evaluation of Language Fundamentals -5 Metalinguistics (up to 22 years of age)
- Semantic Flexibility (e.g., generation of definitions, synonyms, antonyms, multiple meaning words, etc.)
- WORD Test 2 Adolescent (up to 18 years of age)
- Can be supplemented with informal narrative assessment to determine if the student coherently and cohesively summarize expository or narrative texts
- WORD Test 2 Adolescent (up to 18 years of age)
- Critical Thinking and Problem Solving
- TOPS-2 Adolescent Test of Problem Solving-2 (up to 18 years of age)
- Social Communication
- Social Language Development Test Adolescent (up to 18 years of age)
- Clinical Assessment of Pragmatics (CAPs)
- Can be supplemented with informal assessment of social communication Informal Social Thinking Dynamic Assessment Protocol®)
- Executive Function
- Informal use of Situational Awareness STOP Observation Tool (Ward & Jacobsen, 2014)
TESTS OF LITERACY
- Phonological Awareness
- Comprehensive Test of Phonological Processing-2 (CTOPP-2) (up to 25 years of age)
- Word Fluency
- Rapid Automatized Naming/Rapid Alternating Stimulus RAN/RAS (up to 18 years of age)
- Reading Fluency
- GORT-5: Gray Oral Reading Tests−Fifth Edition (up to 24 years of age)
- The Test of Silent Word Reading Fluency (TOSWRF-2) (up to 25 years of age)
- Test of Silent Contextual Reading Fluency (TOSCRF-2) (up to 25 years of age)
- Reading Comprehension
- Spelling
- Writing
- TOWL-4: Test of Written Language–Fourth Edition (up to 18 years of age)
- Can be informally supplemented with the use of Grade Rubrics addressing Persuasive/Expository Texts
- TOWL-4: Test of Written Language–Fourth Edition (up to 18 years of age)
It is understandable how given the sheer amount of assessment choices some clinicians may feel overwhelmed and be unsure regarding the starting point of an adolescent evaluation. Consequently, the use the checklist prior to the initiation of assessment may be highly useful in order to identify potential language weaknesses/deficits the students might experience. It will also allow clinicians to prioritize the hierarchy of testing instruments to use during the assessment.
While clinicians are encouraged to develop such checklists for their personal use, those who lack time and opportunity can locate a number of already available checklists on the market.
For example, the comprehensive 6-page Speech Language Assessment Checklist for Adolescents (below) can be given to caregivers, classroom teachers, and even older students in order to check off the most pressing difficulties the student is experiencing in an academic setting.
It is important for several individuals to fill out this checklist to ensure consistency of deficits, prior to determining whether an assessment is warranted in the first place and if so, which assessment areas need to be targeted.
Checklist Categories:
- Receptive Language

- Memory, Attention and Cognition
- Expressive Language
- Vocabulary
- Discourse
- Speech
- Voice
- Prosody
- Resonance
- Reading
- Writing
- Problem Solving
- Pragmatic Language Skills
- Social Emotional Development
- Executive Functioning

Based on the checklist administration SLPs can reliably pinpoint the student’s areas of deficits without needless administration of unrelated/unnecessary testing instruments. For example, if a student presents with deficits in the areas of problem solving and social pragmatic functioning the administration of a general language test such as the Clinical Evaluation of Language Fundamentals® – Fifth Edition (CELF-5) would NOT be functional (especially if the previous administration of educational testing did not reveal any red flags). In contrast, the administration of such tests as Test Of Problem Solving 2 Adolescent and Social Language Development Test Adolescent would be better reflective of the student’s deficits in the above areas. (Checklist HERE; checklist sample HERE).
It is very important to understand that students presenting with language and literacy deficits will not outgrow these deficits on their own. While there may be “a time period when the students with early language disorders seem to catch up with their typically developing peers” (e.g., illusory recovery) by undergoing a “spurt” in language learning”(Sun & Wallach, 2014). These spurts are typically followed by a “post-spurt plateau”. This is because due to the ongoing challenges and an increase in academic demands “many children with early language disorders fail to “outgrow” these difficulties or catch up with their typically developing peers”(Sun & Wallach, 2014). As such many adolescents “may not show academic or language-related learning difficulties until linguistic and cognitive demands of the task increase and exceed their limited abilities” (Sun & Wallach, 2014). Consequently, SLPs must consider the “underlying deficits that may be masked by early oral language development” and “evaluate a child’s language abilities in all modalities, including pre-literacy, literacy, and metalinguistic skills” (Sun & Wallach, 2014).
References:
- Hill, J. W., & Coufal, K. L. (2005). Emotional/behavioral disorders: A retrospective examination of social skills, linguistics, and student outcomes. Communication Disorders Quarterly, 27(1), 33–46.
- Sun, L & Wallach G (2014) Language Disorders Are Learning Disabilities: Challenges on the Divergent and Diverse Paths to Language Learning Disability. Topics in Language Disorders, Vol. 34; (1), pp 25–38.
Helpful Smart Speech Therapy Resources
- Assessment of Adolescents with Language and Literacy Impairments in Speech Language Pathology
- Assessment and Treatment Bundles
- Social Communication Materials
- Multicultural Materials
Comprehensive Assessment of Elementary Aged Children with Subtle Language and Literacy Deficits
 Lately, I’ve been seeing more and more posts on social media asking for testing suggestions for students who exhibit subtle language-based difficulties. Many of these children are typically referred for initial assessments or reassessments as part of advocate/attorney involved cases, while others are being assessed due to the parental insistence that something “is not quite right” with their language and literacy abilities, even in the presence of “good grades.” Continue reading Comprehensive Assessment of Elementary Aged Children with Subtle Language and Literacy Deficits
Lately, I’ve been seeing more and more posts on social media asking for testing suggestions for students who exhibit subtle language-based difficulties. Many of these children are typically referred for initial assessments or reassessments as part of advocate/attorney involved cases, while others are being assessed due to the parental insistence that something “is not quite right” with their language and literacy abilities, even in the presence of “good grades.” Continue reading Comprehensive Assessment of Elementary Aged Children with Subtle Language and Literacy Deficits
Measurement and Interpretation of Standardized Reading Assessments for Professionals and Parents

New Product Giveaway: Comprehensive Literacy Checklist For School-Aged Children
 I wanted to start the new year right by giving away a few copies of a new checklist I recently created entitled: “Comprehensive Literacy Checklist For School-Aged Children“.
I wanted to start the new year right by giving away a few copies of a new checklist I recently created entitled: “Comprehensive Literacy Checklist For School-Aged Children“.
It was created to assist Speech Language Pathologists (SLPs) in the decision-making process of how to identify deficit areas and select assessment instruments to prioritize a literacy assessment for school aged children.
The goal is to eliminate administration of unnecessary or irrelevant tests and focus on the administration of instruments directly targeting the specific areas of difficulty that the student presents with.
*For the purpose of this product, the term “literacy checklist” rather than “dyslexia checklist” is used throughout this document to refer to any deficits in the areas of reading, writing, and spelling that the child may present with in order to identify any possible difficulties the child may present with, in the areas of literacy as well as language.
This checklist can be used for multiple purposes.
1. To identify areas of deficits the child presents with for targeted assessment purposes
2. To highlight areas of strengths (rather than deficits only) the child presents with pre or post intervention
3. To highlight residual deficits for intervention purpose in children already receiving therapy services without further reassessment
Checklist Contents:
- Page 1 Title
- Page 2 Directions
- Pages 3-9 Checklist
- Page 10 Select Tests of Reading, Spelling, and Writing for School-Aged Children
- Pages 11-12 Helpful Smart Speech Therapy Materials
Checklist Areas:
- AT RISK FAMILY HISTORY
- AT RISK DEVELOPMENTAL HISTORY
- BEHAVIORAL MANIFESTATIONS
- LEARNING DEFICITS
- Memory for Sequences
- Vocabulary Knowledge
- Narrative Production
- Phonological Awareness
- Phonics
- Morphological Awareness
- Reading Fluency
- Reading Comprehension
- Spelling
- Writing Conventions
- Writing Composition
- Handwriting
You can find this product in my online store HERE.
Would you like to check it out in action? I’ll be giving away two copies of the checklist in a Rafflecopter Giveaway to two winners. So enter today to win your own copy!