 In both of the settings where I work, psychiatric outpatient school as well as private practice, I spend a fair amount of time reviewing speech language evaluation reports. As I’m looking at these reports I am seeing that many examiners choose to base their decision making with respect to speech language services eligibility on the students’ core, index, or total scores, which are composite scores. For those who are not familiar with this term, composite scores are standard scores based on the sum of various test scaled scores.
In both of the settings where I work, psychiatric outpatient school as well as private practice, I spend a fair amount of time reviewing speech language evaluation reports. As I’m looking at these reports I am seeing that many examiners choose to base their decision making with respect to speech language services eligibility on the students’ core, index, or total scores, which are composite scores. For those who are not familiar with this term, composite scores are standard scores based on the sum of various test scaled scores.
When the student displays average abilities on all of the presented subtests, use of composite scores clearly indicates that the child does not present with deficits and thereby is not eligible for therapy services.
The same goes for the reverse, when the child is displaying a pattern of deficits which places their total score well below the average range of functioning. Again, it indicates that the child is performing poorly and requires therapy services.
However, there’s also a the third scenario, which presents a cause for concern namely, when the students display a pattern of strengths and weaknesses on a variety of subtests, but end up with an average/low average total scores, making them ineligible for services.
Results of the Test of Problem Solving -2 Elementary (TOPS-3)
| Subtests | Raw Score | Standard Score | Percentile Rank | Description |
| Making Inferences | 19 | 83 | 12 | Below Average |
| Sequencing | 22 | 86 | 17 | Low Average |
| Negative Questions | 21 | 95 | 38 | Average |
| Problem Solving | 21 | 90 | 26 | Average |
| Predicting | 18 | 92 | 29 | Average |
| Determining Causes | 13 | 82 | 11 | Below Average |
| Total Test | 114 | 86 | 18 | Low Average |
Results of the Test of Reading Comprehension-Fourth Edition (TORC-4)
| Subtests | Raw Score | Standard Score | Percentile Rank | Description |
| Relational Vocabulary | 24 | 9 | 37 | Average |
| Sentence Completion | 25 | 9 | 37 | Average |
| Paragraph Construction | 41 | 12 | 75 | Average |
| Text Comprehension | 21 | 7 | 16 | Below Average |
| Contextual Fluency | 86 | 6 | 9 | Below Average |
| Reading Comprehension Index | 90 | Average | ||
The above tables, taken from different evaluations, perfectly illustrate such a scenario. While we see that their total/index scores are within average range, the first student has displayed a pattern of strengths and weaknesses across various subtests of the TOPS-3, while the second one displayed a similar performance pattern on the TORC-4.
Typically in such cases, clinical judgment dictates a number of options:
- Administration of another standardized test further probing into related areas of difficulty (e.g., in such situations the administration of a social pragmatic standardized test may reveal a significant pattern of weaknesses which would confirm student’s eligibility for language therapy services).
- Administration of informal/dynamic assessments/procedures further probing into the student’s critical thinking/verbal reasoning skills.
 Here is the problem though: I only see the above follow-up steps in a small percentage of cases. In the vast majority of cases in which score discrepancies occur, I see the examiners ignoring the weaknesses without follow up. This of course results in the child not qualifying for services.
Here is the problem though: I only see the above follow-up steps in a small percentage of cases. In the vast majority of cases in which score discrepancies occur, I see the examiners ignoring the weaknesses without follow up. This of course results in the child not qualifying for services.
So why do such practices frequently take place? Is it because SLPs want to deny children services? And the answer is NOT at all! The vast majority of SLPs, I have had the pleasure interacting with, are deeply caring and concerned individuals, who only want what’s best for the student in question. Oftentimes, I believe the problem lies with the misinterpretation of/rigid adherence to the state educational code.
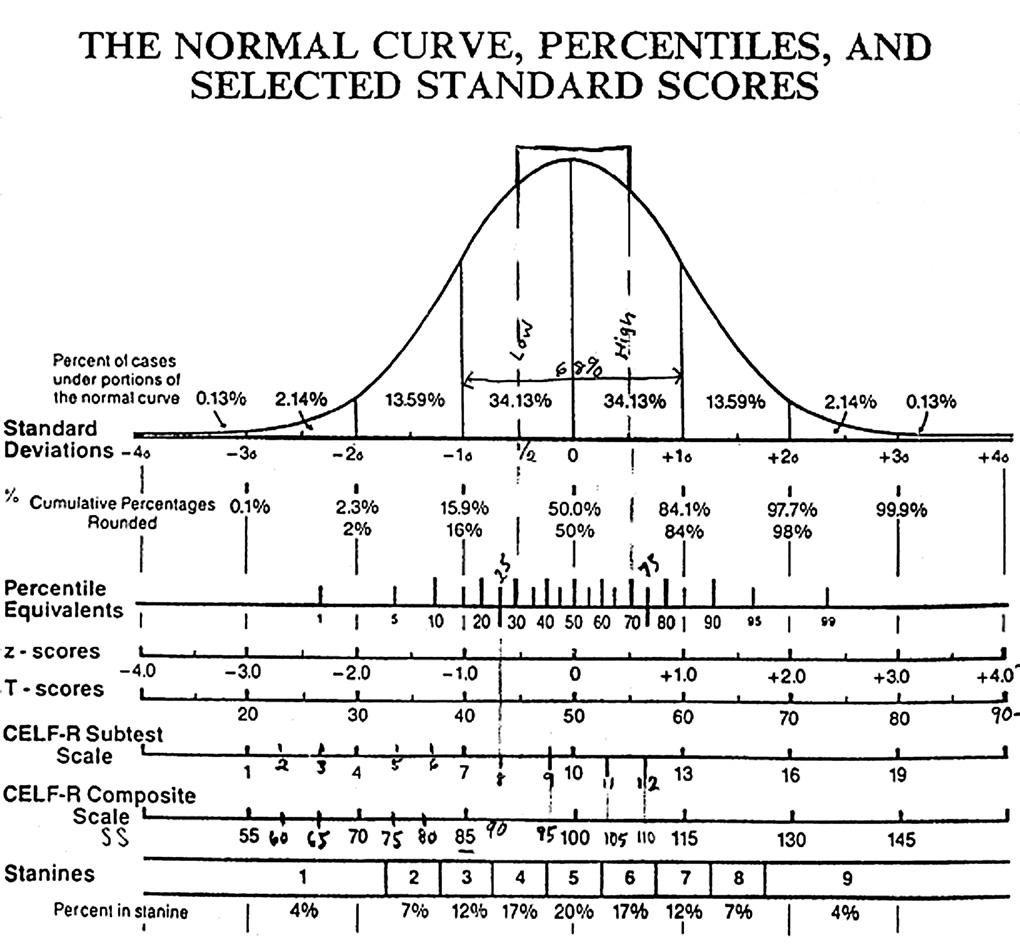
For example, most NJ SLPs know that the New Jersey State Education Code dictates that initial eligibility must be determined via use of two standardized tests on which the student must perform 1.5 standard deviations below the mean (or below the 10th percentile). Based on such phrasing it is reasonable to assume that any child who receives the total scores on two standardized tests above the 10th percentile will not qualify for services. Yet this is completely incorrect!
Let’s take a closer look at the clarification memo issued on October 6, 2015, by the New Jersey Department of Education, in response to NJ Edu Code misinterpretation. Here is what it actually states.
“In accordance with this regulation, when assessing for a language disorder for purposes of determining whether a student meets the criteria for communication impaired, the problem must be demonstrated through functional assessment of language in other than a testing situation and performance below 1.5 standard deviations, or the 10th percentile on at least two standardized language tests, where such tests are appropriate, one of which shall be a comprehensive test of both receptive and expressive language.”
“When implementing the requirement with respect to “standardized language tests,” test selection for evaluation or reevaluation of an individual student is based on various factors, including the student’s ability to participate in the tests, the areas of suspected language difficulties/deficits (e.g., morphology, syntax, semantics, pragmatics/social language) and weaknesses identified during the assessment process which require further testing, etc. With respect to test interpretation and decision-making regarding eligibility for special education and related services and eligibility for speech-language services, the criteria in the above provision do not limit the types of scores that can be considered (e.g., index, subtest, standard score, etc.).”
Firstly, it emphasizes functional assessments. It doesn’t mean that assessments should be exclusively standardized rather it emphasizes the best appropriate procedures for the student in question be they standardized and nonstandardized.
Secondly, it does not limit standardized assessment to 2 tests only. Rather it uses though phrase “at least” to emphasize the minimum of tests needed.
It explicitly makes a reference to following up on any weaknesses displayed by the students during standardized testing in order to get to the root of a problem.
It specifies that SLPs must assess all displayed areas of difficulty (e.g., social communication) rather than assessing general language abilities only.
Finally, it explicitly points out that SLPs cannot limit their testing interpretation to the total scores but must to look at the testing results holistically, taking into consideration the student’s entire assessment performance.
The problem is that if SLPs only look at total/core scores then numerous children with linguistically-based deficits will fall through the cracks. We are talking about children with social communication deficits, children with reading disabilities, children with general language weaknesses, etc. These students may be displaying average total scores but they may also be displaying significant subtest weaknesses. The problem is that unless these weaknesses are accounted for and remediated as they are not going to magically disappear or resolve on their own. In fact both research and clinical judgment dictates that these weaknesses will exacerbate over time and will continue to adversely impact both social communication and academics.
 So the next time you see a pattern of strengths and weaknesses and testing, even if it amounts to a total average score, I urge you to dig deeper. I urge you to investigate why this pattern is displayed in the first place. The same goes for you – parents! If you are looking at average total scores but seeing unexplained weaknesses in select testing areas, start asking questions! Ask the professional to explain why those deficits are occuring and tell them to dig deeper if you are not satisfied with what you are hearing. All students deserve access to FAPE (Free and Appropriate Public Education). This includes access to appropriate therapies, they may need in order to optimally function in the classroom.
So the next time you see a pattern of strengths and weaknesses and testing, even if it amounts to a total average score, I urge you to dig deeper. I urge you to investigate why this pattern is displayed in the first place. The same goes for you – parents! If you are looking at average total scores but seeing unexplained weaknesses in select testing areas, start asking questions! Ask the professional to explain why those deficits are occuring and tell them to dig deeper if you are not satisfied with what you are hearing. All students deserve access to FAPE (Free and Appropriate Public Education). This includes access to appropriate therapies, they may need in order to optimally function in the classroom.
I urge my fellow SLP’s to carefully study their respective state codes as well as know who they are state educational representatives are. These are the professionals SLPs can contact with questions regarding educational code clarification. For example, the SEACDC Consultant for the state of New Jersey is currently Fran Liebner (phone: 609-984-4955; Fax: 609-292-5558; e-mail: fran.leibner@doe.state.nj.us).
However, the Department of Education is not the only place SLPs can contact in their state. Numerous state associations worked diligently on behalf of SLPs by liaising with the departments of education in order to have access to up to date information pertaining to school services. ASHA also helpfully provides contact information by state HERE.
When it comes to score interpretation, there are a variety of options available to SLPs in addition to the detailed reading of the test manual. We can use them to ensure that the students we serve experience optimal success in both social and academic settings.
Helpful Smart Speech Therapy Resources:
 “Well, the school did their evaluations and he doesn’t qualify for services” tells me a parent of a 3.5 year old, newly admitted private practice client. “I just don’t get it” she says bemusedly, “It is so obvious to anyone who spends even 10 minutes with him that his language is nowhere near other kids his age!” “How can this happen?” she asks frustratedly?
“Well, the school did their evaluations and he doesn’t qualify for services” tells me a parent of a 3.5 year old, newly admitted private practice client. “I just don’t get it” she says bemusedly, “It is so obvious to anyone who spends even 10 minutes with him that his language is nowhere near other kids his age!” “How can this happen?” she asks frustratedly?


 As per NJAC 6A:14-2.5
As per NJAC 6A:14-2.5  These delays can be receptive (listening) or expressive (speaking) and need not be based on a total test score but rather on all testing findings with a minimum of at least two assessments being performed. A determination of adverse impact in academic and non-academic areas (e.g., social functioning) needs to take place in order for special education and related services be provided. Additionally, a delay in articulation can serve as a basis for consideration of eligibility as well.
These delays can be receptive (listening) or expressive (speaking) and need not be based on a total test score but rather on all testing findings with a minimum of at least two assessments being performed. A determination of adverse impact in academic and non-academic areas (e.g., social functioning) needs to take place in order for special education and related services be provided. Additionally, a delay in articulation can serve as a basis for consideration of eligibility as well. General Language:
General Language:  Pragmatics/Social Communication
Pragmatics/Social Communication Finally, by showing children simple
Finally, by showing children simple 
 As a speech language pathologist (SLP) who works in an outpatient psychiatric school-based setting, I frequently review incoming students previous speech language evaluation reports. There are a number of trends I see in these reports which I have written about in the past as well as planned on writing about in the future.
As a speech language pathologist (SLP) who works in an outpatient psychiatric school-based setting, I frequently review incoming students previous speech language evaluation reports. There are a number of trends I see in these reports which I have written about in the past as well as planned on writing about in the future.





 Today I’d like to officially introduce a new
Today I’d like to officially introduce a new  Today I’m excited to introduce a new product: “
Today I’m excited to introduce a new product: “ Today I’d like to officially introduce a new
Today I’d like to officially introduce a new 
 Typically when asked that question I always tend to recommend that a trained SLP performs a series of tests aimed to determine whether the student presents with reading and writing deficits.
Typically when asked that question I always tend to recommend that a trained SLP performs a series of tests aimed to determine whether the student presents with reading and writing deficits.
{kind=link}